Clinical Practice Article
Trends in acute myocardial infarction between 2018-2021
Tendencias del infarto agudo de miocardio entre 2018 y 2021
Héctor José Pérez Hernández1*
https://orcid.org/0000-0002-4628-7436
Rubén
David Román Robert1
https://orcid.org/0009-0008-2799-6836
Katherine
Susana Hernández Cortés2
https://orcid.org/0000-0001-9293-9450
1Saturnino
Lora Provincial Hospital. Santiago de Cuba, Cuba.
2University
of Medical Sciences. Santiago de Cuba, Cuba.
*Corresponding author. Email: hectorinmunologia@gmail.com
Background:
Acute myocardial infarction (AMI) is a high incidence heart disease with impact
on hospital morbidity and mortality, common cause of admissions and care in
emergency units.
Objective: To describe the annual behavior of AMI.
Methods: Analytical observational study in 1253 patients admitted for
AMI in the period 01/01/2018 to 31/12/2021, at the Saturnino Lora Hospital in
Santiago de Cuba. The following variables were used: Age, sex, hospital stay,
discharge status, use of homeopathic formulations, and location of the ischemic
lesion. For the statistical analysis, the normality of the data distribution
was evaluated, Fischer and Welch t-tests, chi-square, Log-rank test and Kaplan-Meier
curves were used.
Results: 67.99 % of patients were male. The overall case fatality was
10.21 %. Significant differences in age (62.63 ± 0.73 vs. 71.43 ± 2.04; p= 0.0000)
and hospital stay (7.92 ± 0.33 vs. 3.19 ± 0.66; p= 0.0000) were observed between
live vs. deceased discharged patients. Of the deaths, 57.03 % occurred within
48 hours, 32.81 % within 24 hours and 19.53 % within 12 hours of hospital admission.
Using homeopathic formulations was associated with a clinically significant
protective effect.
Conclusions: Incidence increased in 2020, with a tendency to recover
at the end of the period evaluated; inverse trend in relation to mortality;
a clinically significant protective effect was identified in the use of homeopathic
formulations.
Keywords: heart disease; ischemia; myocardial infarction.
Introducción:
El infarto miocárdico agudo (IAM), es una cardiopatía de alta incidencia,
con impacto en la morbimortalidad hospitalaria, causa común de ingresos y atención
en unidades de emergencias.
Objetivo: Describir el comportamiento anual del IAM.
Métodos: Estudio observacional analítico en 1253 pacientes ingresados
por IAM en el período de 01/01/2018 a 31/12/2021, en el Hospital Saturnino Lora
de Santiago de Cuba. Se utilizaron las siguientes variables: Edad, sexo, estancia
hospitalaria, estado al alta, uso de formulaciones homeopáticas y localización
de la lesión isquémica. Para el análisis estadístico se evaluó la normalidad
en la distribución de datos, se utilizaron las pruebas t de Fischer y Welch,
ji cuadrada, el estadístico Log-rank test, junto con las curvas de Kaplan-Meier.
Resultados: El 67,99 % de los pacientes fueron del sexo masculino. La
letalidad general fue del 10,21 %. Entre egresados vivos vs. fallecidos se observaron
diferencias significativas respecto a la edad (62,63 ± 0,73 vs. 71,43 ± 2,04;
p= 0,0000) y la estadía hospitalaria (7,92 ± 0,33 vs. 3,19 ± 0,66; p= 0,0000).
El 57,03 % de los decesos ocurrieron en las primeras 48 horas, el 32,81 % en
las primeras 24 horas y el 19,53 % en las primeras 12 horas de ingreso hospitalario.
Usar formulaciones homeopáticas se relacionó con un efecto protector clínicamente
significativo.
Conclusiones:
La incidencia aumentó en 2020, con tendencia a recuperarse al final del
período evaluado; tendencia inversa en relación a la mortalidad; se identificó
un efecto protector clínicamente significativo en el uso de formulaciones homeopáticas.
Palabras clave: cardiopatía; isquemia; infarto miocárdico.
Received: 10/06/2024
Approved:
13/02/2025
INTRODUCTION
Acute myocardial infarction (AMI) is a heart disease with a high incidence nationally(1,2) and internationally,(3,4,5) constituting a sensitive health problem, responsible for a significant volume of deaths;(6,7) hence it is one of the most common causes of hospital admission and care in emergency medical units.(8)
The genesis of the pathophysiology of AMI is the ischemic compromise of circulation of the coronary artery network. With coronary artery occlusion, the myocardium is deprived of oxygen. Prolonged deprivation of oxygen supply to the myocardium can lead to cell death and myocardial necrosis. Ischemic injury to the myocardium produces regional necrosis and a decrease in cardiac contractile mass. Consequently, decreased ventricular function conditions systemic hypoperfusion.(9) Among the risk factors associated with the disease, advanced age, sedentary lifestyle, and history of AMI stand out.(10)
Most heart attacks are due to underlying coronary artery disease. Patients may experience discomfort or pressure in the chest that may radiate to the neck, jaw, shoulder, or arm. In addition to history and physical examination, myocardial ischemia may be associated with ECG changes and elevated biochemical markers such as cardiac troponins. Myocardial infarction can be "silent" and go unnoticed, or it can be a catastrophic event leading to hemodynamic deterioration and sudden death.(11)
The global prevalence is around 3.8 % in people under 60 years of age, compared to 9.5 % in people over 60 years of age. It has a strong association with the male sex, despite the fact that other studies report a significant reaction with female sex, in equal association with common risk factors, and differences attributed to sedentary lifestyle and metabolic syndrome.(12)
A trend of increasing mortality from AMI has been observed in recent years in Cuba.(13,14) In 2022, 32,872 deaths due to cardiovascular diseases occurred in Cuba, of which 7,992 corresponded to acute myocardial infarction.(1)
The Cuban scenario, due to the declines that occurred at the primary health level, from the hospital scenario, are not recorded differentially in the Health Statistical Yearbook. The national health system has in its network of polyclinics with technical and professional conditions that allow the care of patients with AMI, until their referral to specialized units.
Given the importance of the disease, continuous monitoring is vital for the evaluation of its behavior on a population scale. This is basic for decision-making in healthcare units, favoring the design of resilient systems that are capable of efficient management of the condition, and premise for a reduction in the risk of deaths.
The objective of this study was to describe the annual behavior of the AMI.
METHODS
Design and subjects
Observational, adaptive, analytical, observational study of a series of cases that met the following criteria: (i) Presentation at the emergency medical unit of the Hospital Provincial Saturnino Lora, (ii) presentation in the period between January 2018 and December 2021; (ii) with a diagnosis of acute myocardial infarction confirmed by an acute ischemic pattern on electrocardiogram. These criteria allowed the recording of the cumulative incidence for the period, the total number of patients being 1253. Patients with more than one admission for AMI (n= 46), or patients affected by AMI during an admission for another reason (n= 35) were included.
Variables
The following variables were used: Age, sex, years, fatality, hospital stay (days), condition at discharge (alive or dead), time of death, use of homeopathic formulations, and location of the ischemic lesion by electrocardiographic signs.
In terms of location, a three-level nominal scale was used, with the categories: Mixed, Anterior Wall and Inferior Wall; the first term referring to the extended ischemic lesion with electrical signs in more than 5 leads, thus involving both the anterior and inferior wall. When referring to the variable condition at discharge, it refers to the event of interest for the Survival Analysis: Death (or not), which is periodized in relation to the length of stay of each case; this is an output declared in the medical software.
Procedures
Clinical data were retrieved thanks to the facilities of the hospital data management service GALENCLINICAS 2.0.0 and organized in a digital database using the services of the Microsoft Office Excel calculation platform.
The variables measured were collected from digital records, which in turn are derived from the discharge sheets, a summary of each patient's medical records, issued by the treating physicians. Each case, according to hospital protocols, is discussed collectively, so that diagnostic data, treatments and medical value judgment are reinforced by the collective experience of the medical service.
The organization by age group responds to the particular interests of the research. This organization corresponds to the internationally reported incidence rate, with the 50-69 and 70-85 age groups commonly distinguished as those of greatest interest. The division of the 20-49 age group into 2 groups of 10 years responds to the important internal differences observed. From the age of 85 years onwards, patients were grouped in a separate group. Associated with the stage groups, they were subclassified in relation to sex.
During the study period, standard pharmacological treatment, anti-ischemic load adjustment and thrombolysis were used, depending on the specifics of the case. If necessary, the patient was transferred to the hemodynamics unit of the hospital. Homeopathic treatment was used as an adjuvant to traditional treatment; it was used on demand depending on hospital availability. The use of homeopathic formulations started around the first 12 hours of admission. Aconitum and Arnica montana were used interchangeably, most frequently with the 6c potency. The supplier of all batches is the "Empresa Provincial de Farmacias y Ópticas de Santiago de Cuba".
Processing
For the statistical description, the arithmetic mean and median were used as summary measures of central tendency; standard deviation and variance were used as measures of dispersion. For the summary of qualitative aspects, the results were expressed in percentages. In the statistical analysis, graphical (Q-Q chart) and computational means (Jarque-Bera test and Shapiro-Wilk test in Royston version) were used to determine the normality of the data distribution, as well as to explore statistical significance, Fischer's and Welch's t-tests (quantitative data) were used, as well as the chi-square test in the case of categorical variables. The log-rank test statistic together with Kaplan-Meier curves allowed the assessment of survival, based on the delimitation of days lived (comparable to the variable "hospital stay" in deceased patients); survival up to 15 days after admission was assessed. Assumed a= 0.05 and Hedges' g for effect size estimation. A univariate strategy was used to estimate an index of association using the relative ratio (RR).
Bioethical aspects
This study had the consent of the competent authorities to obtain information from hospital records, complying with the legal regulations in force in Cuba, and conducting the research under the spirit and letter of the Declaration of Helsinki and the Document of Good Clinical Practices for the Americas.(15,16)
RESULTS
In the patients studied, 67.99 % were male; the average age was 63.53 ± 0.71 years, with a length of stay of 7.44 ± 0.32 days. The overall fatality rate recorded was 10.21 %. Only 16.83 % of the lesions were diffuse in location in the electrocardiographic records; 41.50 % and 41.58 % were located in the anterior and inferior wall respectively. The particular characteristics according to year are seen in table 1.
In relation to sex, differences in incidence were observed in relation to age ranges, with a higher incidence in men compared to women in the age range of 31 to 49 years. The highest proportion of cases in both sexes was observed in the age group of 50-69 years. The specific characteristics according to age range with respect to years are seen in table 2.
Both the average age and hospital stay of the discharged patients compared to the deceased were different with a 5 % significance level; however, the estimation of the effect sizes reflects the absence of clinically relevant differences with respect to age (g= 0.1703), the difference being with respect to the length of stay mild (g= 0.3674). Regarding sex or location of the lesion, no differences were observed, as seen in table 3.
Regarding fatality, 57.03 % of deaths occurred in the first 48 hours, 19.53 % in the first 12 hours and 32.81 % in the first 24 hours of hospital admission. Regarding sex, a trend towards a protective effect related to the male gender was observed without these reaching significance (RR= 0.83; 95 % CI: 0.71-0.9; p= 0.3139). The overall survival curve can be seen in figure 1.
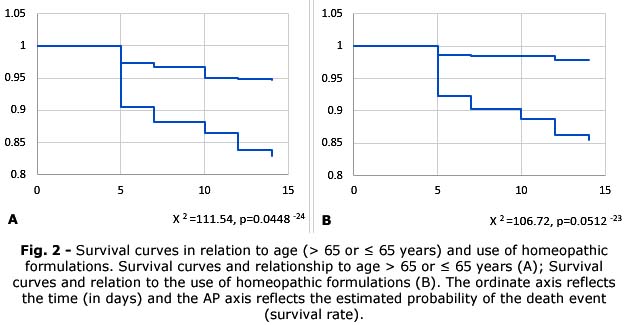
In relation to age, an effect was observed identifying those ages over 65 years behaved as a prognostic factor related to death (RR= 2.69; 95 % CI: 2.27-3.19; p= 0.0388*10-6). The absence of the use of homeopathic formulations behaved as a prognostic factor associated with lethality (RR= 6.55; 95 % CI: 4.83-8.88; p= 0.036*10-8), as can be seen reflected in the survival curves in the figure 2.
DISCUSSION
Acute myocardial infarction, commonly called "heart attack," is a clinical entity of special interest. Given its incidence, it is one of the most frequent causes of emerging demand for medical assistance.(17) As a result of arterial occlusion, massive injury is inflicted on the coronary microcirculation, leading to vascular disintegration and capillary rarefaction in the region of the infarct. Tissue repair after AMI involves a strong angiogenic response that begins at the edge of the infarct and extends to the necrotic core of the infarct.(18) One of the indicators of the immediacy of the repair response is given by local inflammation. The subsequent implications lead to a clinical picture, despite its floridity, commonly typical,(19) that helps a quick presumptive diagnosis.
Despite the existence of modern systems for the diagnosis of AMI, the recording of electrical activity of the heart, technically known as an electrocardiogram (ECG), remains an essential tool to diagnose, stratify risk and guide reperfusion and invasive strategies in patients with suspected acute coronary syndromes. Since its inception in 1902 by Willem Einthoven, the ECG has seen essentially minimal technological advances.(20)
In this study, a progressive increase in lethality over time was observed. The average fatality was around 10% of the subjects treated in the hospital context. The average age is below 65 years. Comparatively, the days of admission were greater in the 2018-2019 biennium vs. 2020-2021. Most declines occurred between 24 and 48 hours of first contact with the secondary health system. Although the incidence is higher in males, mortality was higher in females. Regarding age, age over 65 was significantly related to fatality.
A complete occlusion of the coronary artery represents approximately 30 % of AMI, where the sign of ST segment elevation in the recording of the electrical activity of the heart is a crucial element for the diagnosis. In cases of partial or intermittent occlusion of the artery and are associated with ST segment depressions (~31 %), T wave inversions (~12 %), ST segment depressions, combined with T wave inversions (16 %) or none (~41 %). At an international level, the fatality rate in developed countries is around 9 %, with a reduction to 7 % in relation to the early onset of percutaneous repercussion in AMI with ST segment elevation.(19)
Cardiogenic shock is one of the entities subsequent to AMI, with the greatest association with its lethality. After arterial occlusion until the onset of CS, studies indicate an onset time of around 6.2 (1.7-20.1) as well as earlier at 5.5 (2.3-14.1) hours, with a late onset in about ¼ of the cases.(9,21) This could partially exemplify the possible causes of lethality in the context of the present study.
In the year 2022, in general in the country, 11,428 people died because of a cardiovascular condition of an ischemic nature, of which 69.9 % were specifically an AMI, 29.7 % between 60-79 years old, and a proportion of 57.8 % of men.(1) Pichardo-Ureña J et al.(13) in the Cuban population, have reported that male individuals die from AMI, in proportions that increase with age, but with greater frequency between 70 and 79 years. Contrary to what was reported with a lower degree of consensus,(22,23,24,25) the results of the study differ from what was reported, with a greater lethality in the female sex, in the age group under 70 years of age; in the latter similar to those observed by Gómez J.(26)
The results of García Blas' team outline an age difference associated with the incidence and lethality of AMI, with differences with respect to sex, with older ages associated with female individuals,(27) which is reflected in the results presented.
Rosabal Y et al.(14) in a study carried out at the Center of Cardiology and Cardiovascular Surgery of Santiago de Cuba, based on a sample of 31.5 % of the cases admitted with AMI (selected based on the elevation of the ST segment, the persistence of angina after the use of nitrates and the elevation of serum Troponin levels), have reported a predominance of the male sex, the group of patients aged = 65 years and of lower topography. These results are similar to those observed in current study, although notable divergences are observed in relation to the intensity of the reported differences.
Regarding the location, in the Cuba scenario, as reported, the anterior topography infarction prevails.(28,29,30) Among the different reports, the data provided by Palacio H et al.(31) and Rosabal Y et al.(14) are notable. However, in current study there is no evidence that gives sufficient preponderance to a particular location, and a progressive tendency to increase in diffuse lesions was also observed.
An unexpected and notable finding of the study was the powerful protective effect associated with the use of homeopathic formulations from the beginning of admission. This effect was observed equally in subjects depending on age. The use of homeopathic formulations begins around the first 12 hours of admission. Taking into account that lethality is greater after 24 hours of admission; the protective effect of homeopathic formulations cannot be attributed to a temporal bias related to the presumed state of the patients and its influence on the judgment of the treating physician. This is reinforced given that the use of homeopathic formulations is subject to hospital availability, which gives a partly random character to their use.
There are no sufficient studies regarding the use of homeopathic formulations in the AMI therapeutic scheme. In the case of Golikov A et al.,(32) a potential as a therapeutic adjuvant has been reported based on small format studies, with an association with a lower demand for beta blockers, nitrates, sedatives, angiotensin-converting enzyme inhibitors, without a clear effect on survival.(33)
Despite the large number of patients included, among the limitations of the study, the absence of sufficient humoral data stands out for an analysis with a molecular approach, secondary to the input deficit resulting from the economic pressure measures that Cuba suffers. The exclusion of comorbidities and clinical symptoms from the analysis, because these were not available in the medical software, also limited further depth.
A vulnerability of the hospital data management system is the lack of proportional integration of data and the nonexistence of profiles associated with patients; this limits the ability to keep track of the disease history of each subject, and can lead to underreporting of comorbidities at the time of a new admission.
Other limitations of this study: (i) The logistic coverage, which made it impossible to use biochemical markers for diagnosis during the entire study period; (ii) the patients were analyzed in a restricted study period. Hence the need to develop specific research on the clinical and epidemiological characteristics of patients with criteria for referral to an intensive care unit, in order to achieve a better description of the phenomenon in the province.
However, the established objective is sufficiently fulfilled, and interesting data is provided regarding the behavior of the IMA in the southeastern region of Cuba.
During the study period, the incidence increased in 2020, with a tendency to recover at the end of the period evaluated, with an inverse trend in relation to mortality; a clinically significant protective effect was identified in the use of homeopathic formulations.
BIBLIOGRAPHIC REFERENCES
1. República de Cuba. Ministerio de Salud Pública, Dirección de Registros Médicos y Estadísticas de Salud [Internet]. Anuario Estadístico de Salud 2021. La Habana: MINSAP. 2022. [acceso: 17/04/2024]. Disponible en: https://instituciones.sld.cu/ucmvc/files/2023/10/Anuario-Estad%C3%ADstico-de-Salud-2022-Ed-2023.pdf
2. Vitón-Castillo A, Piñera-Castro H, Guillén-León L, Montes-de-Oca-Carmenaty M, Suárez-López D, Auza-Santiváñez J. Tendencias en la producción científica cubana sobre infarto agudo de miocardio en Scopus [Internet]. Universidad Médica Pinareña. 2022 [acceso: 25/05/2024]; 18(2):e891. Disponible en: https://revgaleno.sld.cu/index.php/ump/article/view/891
3. Gulati R, Behfar A, Narula J, Kanwar A, Lerman A, Cooper L, Singh M. Acute Myocardial Infarction in Young Individuals [Internet]. Mayo Clinic proceedings. 2020; 95(1):136-56. DOI: 10.1016/j.mayocp.2019.05.001
4. Humphries KH, Norris CM, Pilote L. Sex Differences in Acute Myocardial Infarction: Good News and Bad News [Internet]. The Canadian journal of cardiology. 2022; 38(11):1661-3. DOI: 10.1016/j.cjca.2022.08.227
5. Centers for Disease Control and Prevention. Heart Disease Facts [Internet]. Centers for Disease Control and Prevention. 2023. [acceso: 15/04/2024]. Disponible en: https://www.cdc.gov/heartdisease/facts.htm
6. Michaud K, Basso C, d'Amati G, Giordano C, Kholová I, Preston SD, et al. Diagnosis of myocardial infarction at autopsy: AECVP reappraisal in the light of the current clinical classification [Internet]. Virchows Archiv: an international journal of pathology. 2020; 476(2):179-94. DOI: 10.1007/s00428-019-02662-1
7. Damluji AA, Gangasani NR, Grines CL. Mechanical Complication of Acute Myocardial Infarction Secondary to COVID-19 Disease [Internet]. Heart failure clinics. 2023; 19(2):241-9. DOI: 10.1016/j.hfc.2022.08.011
8. Cerón A, Goldstein G. Mortality due to acute myocardial infarction in Guatemala 2018: patterns and inequities [Internet]. Analysis of National Reality Magazine, University of San Carlos of Guatemala. 2018 [acceso: 18/04/2024 ]; 10(201):76-97. Disponible en: http://ipn.usac.edu.gt/wp-content/uploads/2021/03/IPN-RD-201.pdf
9. Samsky MD, Morrow DA, Proudfoot AG, Hochman JS, Thiele H, Rao SV. Cardiogenic Shock After Acute Myocardial Infarction: A Review [Internet]. JAMA. 2021; 326(18):1840-50. DOI: 10.1001/jama.2021.18323
10. DeFilippis AP, Lidani KCF, Nam Y, Trainor PJ, Johnson WC, Heckbert SR, et al. Risk factor associations with individual myocardial infarction subtypes and acute non-ischemic myocardial injury in the Multi-Ethnic Study of Atherosclerosis (MESA): Design and rationale [Internet]. Am Heart J. 2023; 260:151-73. DOI: 10.1016/j.ahj.2023.02.012 ?
11. Ojha N, Dhamoon AS. Myocardial Infarction [Internet]. Treasure Island (FL): StatPearls Publishing. 2024 [acceso: 18/04/2024]. Disponible en: https://pubmed.ncbi.nlm.nih.gov/30725761/
12. Salari N, Morddarvanjoghi F, Abdolmaleki A, Rasoulpoor S, Khaleghi AA, Hezarkhani LA, et al. The global prevalence of myocardial infarction: a systematic review and meta-analysis [Internet]. BMC Cardiovasc Disord. 2023; (1):206. DOI: 10.1186/s12872-023-03231-w
13. Pichardo-Ureña J, Pérez-Sánchez D, Alonso-Herrera A. Caracterización de la mortalidad por infarto agudo de miocardio con elevación del segmento ST en el Hospital Arnaldo Milián Castro (Cuba): Estudio de 6 años [Internet]. CorSalud. 2020 [acceso: 17/04/2024]; 12(3):e693. Disponible en: https://revcorsalud.sld.cu/index.php/cors/article/view/693
14. Rosabal-Garcia Y, Pérez-Infante Y, Rosales-Guibert E, Palacios-Naranjo Y. Caracterización clinicoepidemiológica, ecocardiográfica y terapéutica de pacientes con infarto agudo de miocardio [Internet]. MEDISAN. 2023 [acceso: 17/04/2024]; 27(2):e4381. 15. Disponible en: https://medisan.sld.cu/index.php/san/article/view/4381
World Medical Association. Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Participants [Internet]. JAMA. 2024;23(18): e21972. DOI: 10.1001/jama.2024.21972
16. Organización Panamericana de la Salud. IV Conferencia Panamericana sobre Armonización de la Reglamentación Farmacéutica. República Dominicana 2-4 marzo, 2005. Conclusiones y recomendaciones [Internet]. OPS; 2005. [acceso: 20/04/2024]. Disponible en: https://www.paho.org/es/documentos/iv-conferencia-panamericana-sobre-armonizacion-reglamentacion-farmaceutica-republica-0
17. Mechanic OJ, Gavin M, Grossman SA. Acute Myocardial Infarction [Internet]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 [acceso: 17/04/2024]. Disponible en: https://pubmed.ncbi.nlm.nih.gov/29083808/
18. Wu X, Reboll MR, Korf-Klingebiel M, Wollert KC. Angiogenesis after acute myocardial infarction [Internet]. Cardiovasc Res. 2021; 117(5):1257-73. DOI: 10.1093/cvr/cvaa287
19. Bhatt DL, Lopes RD, Harrington RA. Diagnosis and Treatment of Acute Coronary Syndromes: A Review [Internet]. JAMA. 2022; 327(7):662-75. DOI: 10.1001/jama.2022.0358
20. Birnbaum Y, Rankinen J, Jneid H, Atar D, Nikus K. The Role of ECG in the Diagnosis and Risk Stratification of Acute Coronary Syndromes: an Old but Indispensable Tool [Internet]. Curr Cardiol Rep. 2022; 24(2):109-18. DOI: 10.1007/s11886-021-01628-7
21. Webb JG, Sleeper LA, Buller CE, et al. Implicaciones del momento de aparición del shock cardiogénico después de un infarto agudo de miocardio: un informe del Registro de ensayos SHOCK [Internet]. J Am Coll Cardiol. 2000; 36(3):1084-90. DOI: 10.1016/S0735-1097(00)00876-7pp1084-1090
22. Mnatzaganian G, Braitberg G, Hiller JE, Kuhn L, Chapman R. Sex differences in in-hospital mortality following a first acute myocardial infarction: symptomatology, delayed presentation, and hospital setting [Internet]. BMC Cardiovasc Disord. 2016; 16(1):109. DOI: 10.1186/s12872-016-0276-5
23. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Documento de consenso de expertos. Tercera definición universal del infarto de miocardio [Internet]. Rev Esp Cardiol. 2013 [acceso: 20/04/2024]; 66(2):132.e1-e15. Disponible en: https://www.academia.edu/download/89640938/index.pdf
24. Nguyen HL, Bui QT, Tran HV, Hoang MV, Le TT, Ha DA, et al. Characteristics, in-hospital management, and complications of acute myocardial infarction in northern and Central Vietnam [Internet]. Int J Cardiol. 2022 [acceso: 20/04/2024]; 364:133-8. Disponible en: https://www.sciencedirect.com/science/article/pii/S0167527322009-433?via%3Dihub
25. Wereski R, Kimenai DM, Bularga A, Taggart C, Lowe DJ, Mills NL, et al. Risk factors for type 1 and type 2 myocardial infarction [Internet]. Eur Heart J. 2022 [acceso: 20/04/2024]; 43(2):127-35. Disponible en: https://academic.oup.com/eurheartj/article/43/2/127/6357312?login=false
26. Gómez J. Predictores de mortalidad intrahospitalaria en infarto agudo al miocardio con elevación del segmento ST [Internet]. Rev Med (Col Méd Cir Guatem). 2022 [acceso: 20/04/2024]; 161(1):16-23. Disponible en: https://www.revistamedicagt.org/index.php/RevMedGuatemala/artic-le/view/451/631
27. García Blas S, Cordero A, Diez Villanueva P, Martínez Avial M, Ayesta A, Ariza Sole A, et al. Acute coronary syndrome in the older patient [Internet]. J Clin Med. 2021; 10(18):4132. DOI: 10.3390/jcm10184132
28. Creagh Cazull A, Cazull Imbert I, Márquez Fernández A, Hernández Heredia R, Delfino Vega EL. Factores predictores de mortalidad hospitalaria en pacientes con infarto agudo del miocardio [Internet]. Rev Inf Cient. 2021 [acceso: 23/04/2024]; 100(2):e3339. Disponible en: https://revinfcientifica.sld.cu/index.php/ric/article/view/3339
29. Santos Medina M, Borrero Escobar EM, Cruz Fernández Y, Rodríguez Ramos M, Martínez García G, Mata Cuevas LA. Infarto agudo de miocardio en pacientes diabéticos según niveles de glucemia al ingreso, un estudio multicéntrico [Internet]. Electron Rev "Dr. Zoilo E. Marinello Vidaurreta". 2022 [acceso: 20/04/2024]; 47(4):e3148. Disponible en: https://revzoilomarinello.sld.cu/index.php/zmv/article/view/3148
30. Enamorado Anaya AR, Yero García RO, Ruiz Manzanares A, García Cañete IM, Goro G. Factores pronósticos de mortalidad intrahospitalaria en pacientes con infarto agudo del miocardio con elevación del segmento ST tipo I [Internet]. Rev Inf Cient. 2021 [acceso: 20/04/2024]; 100(1):e3248. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-99332021000100005
31. Palacio Pérez H, Rey García KB, Castillo Cuello JJ. Factores pronósticos de fallo de trombólisis en pacientes con diagnóstico de infarto agudo de miocardio [Internet]. Medicentro Electrónica. 2022 [acceso: 20/04/2024]; 26(4):853-65. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30432022000400853
32. Golikov AP, Babaian IS. Pumpan pri lechenii ishemicheskoi bolezni serdtsa v sochetanii s arterial'noi gipertoniei. Pumpan in the treatment of ischemic heart disease associated with arterial hypertension [Internet]. Ter Arkh. 2001 [acceso: 20/04/2024]; 73(10):68-9. Disponible en: https://pubmed.ncbi.nlm.nih.gov/11763522/
33. Krasnitskii VB, Aronov DM, Zhidko NI. Vliianie complex preparation "Pumpan" in perenosimost' fizicheskikh nagruzok i klinicheskoe techenie ishemicheskoi bolezni serdtsa [Effect of a compound preparation pumpan on exercise tolerance and clinical course of ischemic heart disease] [Internet]. Ter Arkh. 2003 [acceso: 20/04/2024]; 75(8):17-21. Disponible en: https://pubmed.ncbi.nlm.nih.gov/14520844/
Conflict of interest
Neither the authors nor the related institution received remuneration or other incentives for carrying out this study.
Funding
No funding was received for this study.
Authorship contribution
Conceptualization: Héctor José Pérez Hernández.
Data
curation: Héctor José Pérez Hernández, Rubén David Román Robert, Katherine
Susana Hernández Cortés.
Formal
analysis: Héctor José Pérez Hernández, Rubén David Román Robert, Katherine
Susana Hernández Cortés.
Research:
Héctor José Pérez Hernández, Rubén David Román Robert, Katherine Susana
Hernández Cortés.
Methodology:
Héctor José Pérez Hernández, Rubén David Román Robert, Katherine Susana
Hernández Cortés.
Resources:
Not applicable
Supervision:
Héctor José Pérez Hernández, Katherine Susana Hernández Cortés.
Validation:
Héctor José Pérez Hernández, Katherine Susana Hernández Cortés.
Visualization:
Héctor José Pérez Hernández, Katherine Susana Hernández Cortés.
Writing
- original draft: Héctor José Pérez Hernández, Rubén David Román Robert,
Katherine Susana Hernández Cortés.
Writing
- review and editing: Héctor José Pérez Hernández, Rubén David Román Robert,
Katherine Susana Hernández Cortés.
Data availability statement
The study data are confidential. To access them, authorization is required from the General Management of the Saturnino Lora Provincial Hospital.