Research Article
Oral hygiene in troop personnel of a Peruvian barracks
Higiene oral en el personal de tropa de un cuartel peruano
Susan Belén Yanapa-Vilca1* https://orcid.org/0000-0003-4044-4290
1Universidad Nacional “Jorge Basadre Grohmann”. Tacna, Perú.
*Correspondencia. Correo electrónico: syanapavilca@gmail.com
ABSTRACT
Introduction: Oral hygiene is essential to prevent oral diseases and maintain general health. In the military context, good oral hygiene is crucial because of its impact on troop performance.
Objective: To determine the level of oral hygiene among the troops of the "Fuerte Arica" barracks in Tacna.
Methodology: Descriptive study with a quantitative and cross-sectional approach. Age, education level and military grade were considered. The 394 military personnel participated and the Simplified Oral Hygiene Index (OHI-S) was used, using plaque-revealing tablets. The data were organized in Microsoft Excel and processed in IBM SPSS Statistics 26, using the non-parametric Kruskal-Wallis test.
Results: 59.9% of the military had a regular level of oral hygiene, 29.9% a poor level and 10.2% a good level. According to age, 57.7% of military personnel aged 18-21 and 74.3% of 22-25 years had a regular level, and 60% of military personnel aged 26-30 years old had a good level. According to the level of education, 68.6% with primary education had a poor level, 67% with secondary education had a regular level and 56.3% with higher education had a good level. According to the military rank; soldiers, corporals, second and first sergeants had a regular level, in the same order, with percentages of 54.5%, 69.4%, 66.1% and 76.5%.
Conclusion: It was determined that the troop personnel of the "Fort Arica" barracks in Tacna had a regular level of oral hygiene.
Keywords: military personnel; oral hygiene; oral hygiene index.
RESUMEN
Introducción: La higiene oral es esencial para prevenir enfermedades bucales y mantener la salud general. En el contexto militar, una buena higiene oral es crucial, debido a su impacto en el rendimiento del personal de tropas.
Objetivo: Determinar el nivel de higiene oral en el personal de tropas del cuartel “Fuerte Arica”, en Tacna.
Metodología: Estudio descriptivo cuantitativo y transversal. Se consideraron: edad, grado de instrucción y grado militar. Participaron 394 militares; se utilizó el Índice de Higiene Oral Simplificado (OHI-S) empleando pastillas reveladoras de placa. Los datos se organizaron en Microsoft Excel y se procesaron en IBM-SPSS Statistic v.26. Se utilizó la prueba no paramétrica de Kruskal-Wallis.
Resultados: El 59,9 % presentó un nivel de higiene oral regular, 29,9 % nivel malo y 10,2 % bueno. Según la edad, el 57,7 % de 18 a 21 años y el 74,3 % de 22 a 25 años, presentó nivel regular; el 60 % de 26 a 30 años y un nivel bueno. Según grado de instrucción, el 68,6 % con educación primaria tuvo nivel malo; el 67 % con educación secundaria, un nivel regular, y el 56,3 % con educación superior, bueno. Según el grado militar, los soldados, cabos, sargentos segundos y primeros presentaron nivel regular, en ese orden, con porcentajes de 54,5 %, 69,4 %, 66,1 % y 76,5 %.
Conclusión: Se determinó que el personal de tropa del cuartel “Fuerte Arica” en Tacna presentó un nivel de higiene oral regular.
Palabras clave: higiene bucal; índice de higiene oral; personal militar.
Received: 14/11/2024
Approved: 28/07/2025
INTRODUCTION
Oral hygiene is the set of practices designed to keep the mouth free from disease, mainly by removing the dental biofilm, a layer of microorganisms that sticks to teeth and gums. If not properly controlled, it can lead to caries, periodontal disease and other oral health complications.(1,2) Inadequate oral hygiene could have serious consequences, such as tooth loss, halitosis and systemic impairment.(3,4)
The relationship between oral health and general health has become increasingly evident in recent years. Research has shown that poor oral health, particularly periodontal disease, is associated with a higher incidence of chronic conditions such as cardiovascular disease, diabetes, respiratory infections, and pregnancy complications, including premature birth and low birth weight.(5,6,7,8) Additionally, oral health problems can negatively affect people's quality of life, causing pain, difficulty eating and speaking, and impacting self-esteem and social relationships.(9,10)
In the armed forces, maintaining optimal health is of paramount importance as it directly influences the operational capability of the military. Proper oral hygiene is essential in this context, not only to prevent disease but also to ensure that staff are in the best condition to fulfil their responsibilities.(11) In epidemiological studies, the simplified oral hygiene index (OHI-S) is one of the most widely used indicators for assessing oral health and was used in this study to measure the level of oral hygiene among military personnel.(12,13) Also, factors such as age, level of education and military rank can significantly influence oral hygiene habits and the prevalence of oral diseases in this population.(14,15)
Given the importance of oral hygiene for general health and its preventive role against oral diseases, particularly caries and periodontal diseases—both of which have been linked to systemic conditions in recent years—this study aimed to evaluate the oral hygiene levels of soldiers at the "Fuerte Arica" Barracks in Tacna, Peru, and to examine their relationship with factors such as age, education level, and military rank, in order to provide data for a better understanding of the oral health epidemiological situation within this population.
METHODS
Design
A descriptive study was carried out with a non-experimental, transversal and quantitative design to evaluate the level of oral hygiene among the personnel of the "Fuerte Arica" barracks in Tacna; the variables age, educational level and military rank were also considered.
Subjects
The study included all military personnel who performed their voluntary service in 2023, with a total of 394 participants, all of whom were adults aged between 18 and 30 years, in accordance with Peruvian regulations. The following selection criteria were applied:
Inclusion criteria: Personnel of the troop who signed the informed consent.
Exclusion criteria: Troops with orthodontic appliances and/or who use dental prostheses.
Variables
The level of oral hygiene was evaluated as the main variable, supplemented with demographic variables such as age, educational level and military rank, to achieve the study objectives.
Procedures
The main instrument was the Simplified Oral Hygiene Index (OHI-S), which was recorded in a detailed data collection sheet.
To improve the accuracy of plaque detection and more reliably record the oral hygiene index, a plaque-revealing tablet was used. The use of these tablets is scientifically supported, as they selectively dye plaque, facilitating its visualization and quantification. This allows for a more objective and detailed assessment of plaque-buildup areas, improving the accuracy of the oral hygiene index obtained and minimizing the risk of underestimating plaque levels. The data collected was tabulated in Microsoft Excel for preliminary organization.
Processing
The data were processed using IBM SPSS Statistics version 26 software, employing descriptive statistical measures such as frequencies and percentages to analyze the level of oral hygiene in the sample and its demographic characteristics. To assess the normality of the data, the Kolmogorov-Smirnov test was applied. Since the data did not follow a normal distribution, the non-parametric Kruskal-Wallis test was used to determine if there was a statistically significant relationship between oral hygiene, age, education level, and military rank.
Bioethical aspects
The study followed the ethical principles set out in the World Medical Declaration Declaration of Helsinki for human medical research. The Jorge Basadre Grohmann National University from Tacna, Perú approved its implementation. Informed consent was requested from all participants, ensuring the confidentiality of the information recorded. The participants' names were not identified at any time during the study.
RESULTS
Figure 1 shows that the level of oral hygiene among the troops in the "Fuerte Arica" barracks is predominantly regular, at 59.9 percent (n = 236).
Figure 2 shows that the regular level of oral hygiene was predominant among military personnel aged 18-21 years with 57.7% (n = 179), and 74.3% (n = 55) for those aged 22-25, unlike the ranks of 26 to 30-year-old men, who had a good level of 60.0% (n = 6).
Figure 3 shows that among the primary school-educated military personnel, a poor level of oral hygiene prevailed at 68.6% (n = 35); 67.0% (n = 219) of the secondary school-educated military personnel had a regular level. The majority of those with a university or technical education had a good level, 56.3% (n = 9).
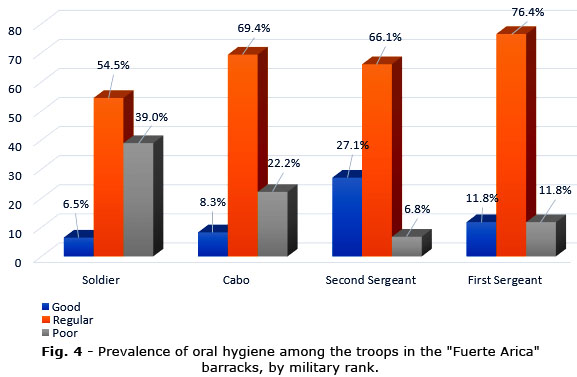
Figure 4 shows that both soldiers, corporals, second and first sergeants had a predominance of regular oral hygiene with 54.5% (n = 134), 69.4% (n = 50), 66.1% (n = 39) and 76.5% (n = 13) respectively.
Table 1 shows that the results of the non-parametric Kruskal-Wallis test, with p-values below 0.05, reveal statistically significant differences in oral hygiene levels according to age, the educational level and military rank of soldiers.
DISCUSSION
Oral hygiene is an important part of health care and is crucial to preventing diseases like dental caries and periodontal disease. The results of this study show that 59.9% of the troops had a regular level of oral hygiene, 29.9% a poor level and 10.2% a good level. These results are similar to those found by Pardo S(16) when studying military volunteer service personnel of the Peruvian Army Commandos School in Lima, identifying that 58.7% had a regular level of oral hygiene, 21.7% a poor level and 19.6% a good level. Similarly, Solórzano K(17) when he studied the level of oral hygiene in military personnel aged 18 to 25 from a barracks in Puno, determined that 40.24% of the military had a regular level of oral hygiene, 36.59% showed a poor level and 23.17% a good level. It also resembles the study by Mego J(18) which, in its research carried out on military personnel attending the Army’s dental clinic in Lambayeque, found that 81.1% had a regular level of oral hygiene, 16.8% a poor level and 2.1% a good level.
In contrast to the findings of this research, the study by Paricoto N(19) made in 40 military personnel found that 60% had a poor level of oral hygiene, 30% a regular level and 10% a good level. Similarly, in the Monge P(20) study, it was found that 75% had a poor level of oral hygiene, 15% a regular level and 10% a good level. Similarly, the results of Marca Y(21), which found a poor level of oral hygiene in 91.3%, questionable in 7.7% and acceptable in 1.0% of military personnel.
The difference between the results obtained by the first two studies may be due to the lower number of military personnel studied by these researchers and the age difference in the populations chosen.(19,20) The disparity in results with the study by the last author is due to the fact that in its research it used the O'leary index.(21)
With regard to age, the results show that the youngest military members, aged 18-21 and 22-25, had a regular level of oral hygiene, represented by 57.7% and 74.3%, respectively, while 60% of military personnel aged 26 to 30 showed a good level. The difference found between age groups was statistically significant (p = 0.014), which suggests that age could influence oral hygiene levels among military personnel. These results coincide with those found by Solórzano K(17) where military men aged 22 to 25 years old achieved a regular level of oral hygiene (69.4%); however, they differ in terms of the military men aged 18 to 21 years old, who showed a poor level of oral hygiene with 78.9%. In addition, the results of this study, which show good oral hygiene among military personnel over 26 years old, suggest that with age and maturity, soldiers tend to be more aware of the negative effects of not maintaining proper hygiene. The early development stage of younger military personnel may be related to neglect of personal hygiene, as has been shown in other studies where lack of responsibility and awareness about oral health prevail at this stage.(16, 17) The high prevalence of periodontal disease in these groups is an additional factor related to poor oral hygiene, tobacco consumption and poor dental care.(22) In contrast, older military personnel are more aware of the potential damage that oral problems can cause in the long term.(16)
In relation to educational level, staff with university or technical education had a much higher percentage of good oral hygiene than those with primary or secondary education. 68.6 percent of the troops with primary education had a poor level of oral hygiene, 67 percent with secondary education had a regular level, and 56.3 percent with university or technical education had a good level. The difference observed between groups was also statistically significant (p = 0.001), which suggests that education level has a major impact on oral hygiene. These results are consistent with previous studies that indicate that higher education is related to better oral hygiene practices.(23) Similarly, research such as that of King S et al.(24) in Australia has suggested that lack of knowledge about oral health may result from participants' low autonomy over their own health, a situation which is exacerbated by social and educational disadvantages. This type of inequality was reflected in a study where 45% of the population reached only secondary education.
As for military rank, the level of oral hygiene was regular in all ranks of the troops: 54.5% for soldiers, 69.4% for corporals, 66.1% for second sergeants and 76.5% for first sergeants. However, it was in the lower ranks that a higher percentage of poor oral hygiene was found, compared to sergeants. The difference observed between the ranges was statistically significant (p = 0.001), indicating that the range could be associated with the level of oral hygiene.
These results are similar to those found by Van Klink N(25) who noted that the lower ranges showed worse oral hygiene levels than those of higher ranges. This phenomenon may be related to the reduced access to health services, as lower-ranking soldiers often have fewer opportunities to go to the Military Health Centre. In addition, the frequent rotation of these soldiers may influence poor adherence to preventive oral health practices.(26,27,28)
One of the limitations of the study was restricted access to officers and non-commissioned officers, which restricted the sample to uniformed personnel only. This limitation may affect the generalization of results, as higher ranks might have different habits due to factors such as increased access to resources and greater awareness of the importance of oral hygiene. Despite this limitation, the study provides relevant information on oral hygiene levels among military personnel, contributing to limited knowledge about oral health practices in the military population in Peru. The use of the simplified oral hygiene index (OHI-S) has added reliability to the results obtained.
In conclusion, the results highlight the need to implement specific oral health programs within the military, especially aimed at lower-ranking personnel and younger age groups with deficiencies in their oral hygiene. It is essential to promote continuing oral health education, through regular workshops, adapted to the needs of military personnel due to their constant rotation. Improving access to dental care and increasing awareness of oral hygiene could significantly reduce the prevalence of periodontal disease and other oral conditions in this population. Future studies should include a wider spectrum of military personnel, including officers and non-commissioned officers, to gain a more complete picture of oral hygiene practices in different ranks. In addition, it would be useful to further explore the relationship between education and oral health, considering the impact of vocational education and health training.
Acknowledgements
To Dr. Ulises Peñaloza for his invaluable advice, guidance and support during the realization of this work.
BIBLIOGRAPHIC REFERENCES
1. Martignon S, Roncalli A, Alvarez E, Aránguiz V, Feldens C, Rabelo M. Risk factors for dental caries in Latin American and Caribbean countries [Internet]. Braz Oral Res. 2021 [acceso: 01/10/2024]; 35(1):28. Disponible en: https://pubmed.ncbi.nlm.nih.gov/34076077/
2. Cho Y, Kim K, Lee Y, Ku Y, Seol Y. Oral Microbiome and Host Health: Review on Current Advances in Genome-Wide Analysis [Internet]. Appl Sci. 2021 [acceso: 01/10/2024]; 11(9):4050. Disponible en: https://www.mdpi.com/2076-3417/11/9/4050
3. Li Z, Li J, Fu R, Liu J, Wen X, Zhang L. Halitosis: etiology, prevention, and the role of microbiota [Internet]. Clin Oral Investig. 2023 [acceso: 25/10/2024]; 27(11):6383-93. Disponible en: https://pubmed.ncbi.nlm.nih.gov/37843633/
4. Cardoso D, Couto F, Cardoso A, Bobrowicz-Campos E, Santos L, Rodrigues R, et al. The Effectiveness of an Evidence-Based Practice (EBP) Educational Program on Undergraduate Nursing Students’ EBP Knowledge and Skills: A Cluster Randomized Control Trial [Internet]. Int J Environ Res Public Health. 2021 [acceso: 05/10/2024]; 18(1):293. Disponible en: https://pubmed.ncbi.nlm.nih.gov/33401523/
5. Adebayo E, Abodunrin O, Adewole I, Salako A, Lusher J, Akinsolu F, et al. Oral Diseases and Adverse Pregnancy Outcomes in Sub-Saharan Africa: A Scoping Review. [Internet]. BioMed. 2023 [acceso: 05/10/2024]; 4(1):1-18. Disponible en: https://www.mdpi.com/2673-8430/4/1/1
6. Liccardo D, Cannavo A, Spagnuolo G, Ferrara N, Cittadini A, Rengo C, et al. Periodontal Disease: A Risk Factor for Diabetes and Cardiovascular Disease [Internet]. Int J Mol Sci. 2019 [acceso: 06/10/2024]. Disponible en: https://pubmed.ncbi.nlm.nih.gov/30897827/
7. Sanz M, Del Castillo A, Jepsen S, Gonzalez-Juanatey J, D’Aiuto F, Bouchard P, et al. Periodontitis and cardiovascular diseases: Consensus report [Internet]. J Clin Periodontol. 2020 [acceso: 12/12/2024]. Disponible: https://pubmed.ncbi.nlm.nih.gov/32011025/
8. Nibali L, Gkranias N, Mainas G, Di Pino A. Periodontitis and implant complications in diabetes [Internet]. Periodontol 2000. 2022 [acceso: 12/12/2024]:88-105. Disponible: https://pubmed.ncbi.nlm.nih.gov/35913467/
9. Su N, Wijk A, Visscher C. Psychosocial oral health-related quality of life impact: A systematic review [Internet]. J Oral Rehabil. 2021 [acceso: 06/10/2024]; 48(3):282-92. Disponible en: https://pubmed.ncbi.nlm.nih.gov/32761938/
10. Knorst J, Sfreddo C, Meira G, Zanatta F, Vettore M, Ardenghi T. Socioeconomic status and oral health-related quality of life: A systematic review and meta-analysis [Internet]. Community Dent Oral Epidemiol. 2021 [acceso: 06/10/2024]; 49(2):95-102. Disponible en: https://pubmed.ncbi.nlm.nih.gov/33368600/
11. Azil A, Yusof Z, Marhazlinda J. Clustering of Health and Oral Health-Compromising Behaviours in Army Personnel in Central Peninsular Malaysia [Internet]. Healthcare. 2023 [acceso: 06/10/2024]; 11(5):640. Disponible en: https://www.mdpi.com/2227-9032/11/5/640
12. Gasner N, Schure R. Periodontal Disease [Internet]. Treasure Island: StatPearls; 2024. [acceso: 06/10/2024]. Disponible en: http://www.ncbi.nlm.nih.gov/books/NBK554590/
13. Greene JC, Vermillion JR. The oral hygiene index: a method for classifying oral hygiene status [Internet]. J Am Dent Assoc. 1960 [acceso: 06/10/2024];61:172-9 Disponible en: https://linkinghub.elsevier.com/retrieve/pii/S0002-8177(64)81004-7
14. Barakat F, Fagbule O, Akiloye S, Lawal T, Adremi G. Impact of oral hygiene habits on oral health-related quality of life of in-school adolescents in Ibadan, Nigeria [Internet]. Front Oral Health, 2022. [acceso: 06/10/2024]; 9(3): 979674. Disponible en: https://pubmed.ncbi.nlm.nih.gov/36338573/
15. Bárcena M, Cobo J, Arcos P. Prevalence and severity of periodontal disease among Spanish military personnel [Internet]. BMJ Mil Health. 2022 [acceso: 06/10/2024]; 168(2):132-5. Disponible en: https://pubmed.ncbi.nlm.nih.gov/32139407/
16. Pardo S. Eficacia de un programa promocional preventivo en higiene oral en la escuela de comandos del ejercito del Perú. Lima 2019 [Internet]. [Tesis de maestría]. Perú: Univ Nac Federico Villarreal; 2021. [acceso: 03/10/2024]. Disponible en: https://repositorio.unfv.edu.pe/handle/20.500.13084/5902
17. Solórzano K. Relación entre nivel de conocimiento sobre salud bucal e higiene oral en militares de 18 - 25 años del Cuartel Manco Capac Puno Mayo- Setiembre 2017 [Internet]. [Tesis de pregrado]. Perú: Univ Nac Altiplano; 2018. [acceso: 03/10/2024]. Disponible en: http://repositorio.unap.edu.pe/handle/UNAP/8590
18. Mego J. Relación entre el nivel de conocimiento de salud oral y los hábitos de higiene oral en soldados atendidos en el consultorio odontológico de la sanidad del ejército peruano-Lambayeque, 2016 [Internet]. [Tesis de pregrado]. Perú: Universidad Alas Peruanas; 2018. [acceso: 04/10/2024]. Disponible en: https://repositorio.uap.edu.pe/xmlui/handle/20.500.12990/9337
19. Paricoto N. Efectividad de la educación sobre salud oral en la actitud y el índice de higiene oral en el personal de tropa del Regimiento de Caballería Blindado Mayor Rázuri No 9 Pomata, 2018 [Internet]. [Tesis de pregrado]. Perú: Univ Nac Altiplano; 2020. [acceso: 04/10/2024]. Disponible en: http://repositorioslatinoamericanos.uchile.cl/handle/2250/3279226
20. Monge P. Efecto detergente de las manzanas (Pyrus malus L) y peras (Pyrus communís L.) en la mala higiene oral de los soldados del Ejército del Perú brigada 31a de infantería, Huancayo - 2017 [Internet]. [Tesis de pregrado]. Perú: Universidad Alas Peruanas; 2017. [acceso: 04/10/2024]. Disponible en: https://repositorio.uap.edu.pe/xmlui/handle/20.500.12990/3745
21. Marca Y. Calidad de vida y su relación con la salud bucal en la tropa del cuartel Tarapacá Tacna 2021 [Internet]. [Tesis de pregrado]. Perú: Universidad Alas Peruanas; 2021. [acceso: 04/10/2024]. Disponible en: https://repositorio.uap.edu.pe/xmlui/handle/20.500.12990/9506
22. Noda V, Pimentel B, Cabarrocas F, Fiu E, Álvarez I, Barreras A. La enfermedad periodontal inflamatoria crónica en jóvenes de la Provincia de Villa Clara [Internet]. Acta Médica. 2016 [acceso: 06/10/2024]; 10(3):19-26. Disponible en: https://revactamedicacentro.sld.cu/index.php/amc/article/view/681
23. Lazo L, Cosio H. Higiene oral. Grado de instrucción materna y su asociación con la caries en niños de 6 a 9 años [Internet]. Cienc Desarro. 2016. [acceso: 05/10/20244]; 18(2):47-54. Disponible en: https://revistas.uap.edu.pe/ojs/index.php/CYD/article/view/1079
24. King S, Thaliph A, Laranjo L, Smith B, Eberhard J. Oral health literacy, knowledge and perceptions in a socially and culturally diverse population: a mixed methods study [Internet]. BMC Public Health. 2023 [acceso: 07/10/2024]; 23(1): 1446. Disponible en: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-023-16381-5
25. Van Klink N. Oral Health Disparities in the Royal Netherlands Armed Forces [Internet]. Mil Med. 2022 [acceso: 07/10/2024]; 188(5-6):1054-9. Disponible en: https://pubmed.ncbi.nlm.nih.gov/35043185/
26. Anhuaman K, Sandoval M. Nivel de conocimiento sobre salud bucal en personal militar Puno 2021 [Internet]. [Tesis de pregrado]. Perú: Universidad César Vallejo; 2021. [acceso: 04/10/2024]. Disponible en: https://repositorio.ucv.edu.pe/handle/20.500.12692/75527
27. Gobierno del Perú. Servicio Militar Voluntario [Internet]. Perú: Gobierno; 2024. [acceso: 08/10/2024]. Disponible en: https://www.gob.pe/568-servicio-militar-voluntario
28. Gobierno del Perú. Servicio Militar Voluntario en el Ejército del Perú [Internet]. Perú: Gobierno; 2024. [acceso: 08/10/2024]. Disponible en: https://www.gob.pe/14579-servicio-militar-voluntario-en-el-ejercito-del-peru
Conflicts of interest
The author declares no conflicts of interest in relation to this research.
Financial information
The author declares that it has not received funding for the development of this research.
Contributions from the authors
Sole author.
Availability of data
Complementary file: Research database. Excel 2016. Available from: https://revmedmilitar.sld.cu/index.php/mil/libraryFiles/downloadPublic/81