Research Article
Risk of hereditary spherocytosis misdiagnosis due to limited effective diagnostic methods
Riesgo de diagnóstico erróneo de la esferocitosis hereditaria debido a la limitación de métodos diagnósticos efectivos
Hien Thanh Dao1
https://orcid.org/0009-0000-3368-9631
Triet Hy Van1*
https://orcid.org/0000-0002-3210-140X
Tuyet Thi Bach Tran1
https://orcid.org/0009-0003-0416-3915
Dat Quoc Ngo1
https://orcid.org/0000-0003-1461-0216
Anh Thi Mai Nguyen1
https://orcid.org/0000-0001-8762-0082
1University of Medicine and Pharmacy at Ho Chi Minh City. Ho Chi Minh City, Vietnam.
*Author for correspondence. Email: vanhytriet@ump.edu.vn
ABSTRACT
Introduction: Hereditary spherocytosis is
a prevalent congenital hemolytic erythrocyte membranopathy. Laboratory
diagnosis is traditionally based on erythrocyte morphology, yet 20% of
cases may lack visible spherocytes, leading to misdiagnosis. The
Eosin-5'-maleimide binding assay has emerged as a reliable diagnostic
method.
Objective: Evaluate the effectiveness of Eosin-5'-maleimide binding
assay in diagnosing hereditary spherocytosis in pediatrics with
negative-direct-antiglobulin-test-hemolytic anemia.
Methods: A cross-sectional study was conducted with 66
negative-direct-antiglobulin-test-hemolytic-anemic patients and 44 healthy
controls. The percentage of spherocytes was scored from peripheral blood
smear observation; the percentage of decreased mean fluorescent intensity
from Eosin-5'-maleimide binding assay was used to determine red cell
membrane protein deficiency, and hereditary spherocytosis was finally
confirmed by gene sequencing as a gold standard.
Results: Eosin-5'-maleimide binding assay demonstrated high
sensitivity (93.33%), specificity (100%), and accuracy (97.3%) in detecting
hereditary spherocytosis, with an optimal cut-off value of 47.83% decreased
mean fluorescent intensity.
Conclusion: The Eosin-5'-maleimide binding assay is a highly
accurate diagnostic tool that outperforms traditional blood smear analysis.
It is precious for detecting hereditary spherocytosis in patients with mild
clinical manifestations or coexisting hemolytic disorders. This assay
should be considered a frontline test for diagnosing hereditary
spherocytosis in patients with hemolytic anemia.
Keywords: anemia; flow cytometry; fluorescence; hereditary; spherocytosis.
RESUMEN
Introducción: La esferocitosis hereditaria es una hemoglobinopatía
congénita hemolítica prevalente. El diagnóstico de laboratorio se basa
tradicionalmente en la morfología de los glóbulos rojos; sin embargo, 20 %
de los casos puede no presentar esferocitos visibles, lo que lleva a un
diagnóstico erróneo. La prueba de unión de eosina-5'-maleimida ha emergido
como un método diagnóstico fiable .
Objetivo: Evaluar la efectividad de la prueba de unión de
eosina-5'-maleimida en el diagnóstico de esferocitosis hereditaria en niños
con anemia hemolítica y prueba de-antiglobulina-directa-negativa.
Métodos: Estudio transversal en 66 pacientes con anemia hemolítica
negativa a la prueba antiglobulina directa y 44 controles sanos. El
porcentaje de esferocitos se evaluó mediante la observación de frotis de
sangre periférica; el porcentaje de disminución de la intensidad
fluorescente media, del ensayo de unión a eosina-5'-maleimida se utilizó
para determinar la deficiencia de proteínas de la membrana de los glóbulos
rojos. La esferocitosis hereditaria se confirmó finalmente mediante
secuenciación genética (estándar de oro).
Resultados:La prueba de unión de eosina-5'-maleimida demostró una
alta sensibilidad (93,33 %), especificidad (100 %) y precisión (97,3 %)
para detectar esferocitosis hereditaria, con un valor de corte óptimo de
47,83 % de disminución en la intensidad fluorescente media.
Conclusión: La prueba analizada es una herramienta diagnóstica
precisa que supera al análisis tradicional de frotis de sangre. Es valiosa
para detectar esferocitosis hereditaria en pacientes con manifestaciones
clínicas leves o trastornos hemolíticos coexistentes. Esta prueba debe
considerarse un test de primera línea para el diagnóstico de esferocitosis
hereditaria en pacientes con anemia hemolítica.
Palabras clave: anemia; citometría de flujo; esferocitosis; fluorescencia; hereditaria.
Received: 28/11/2024
Approved: 25/01/2025
INTRODUCTION
Congenital hemolytic anemia (HA) is the most common type of hemolytic disorder, composed of erythrocyte membranopathies, hemoglobinopathies, and erythrocyte enzymopathies.(1) In many erythrocyte membranopathies, the abnormalities of erythrocyte cytoskeleton such as band 3, spectrin and/or ankyrin - also called "skeletal protein" defects - account for the majority of cause. These structure protein deficiencies result in morphologic changes of erythrocytes from biconcave disc to sphere, then the increasing of peripheral blood spherocytes - the hallmark of hereditary spherocytosis (HS) diagnosis in laboratory experiments.
Typical symptoms of severe HS are anemia, jaundice, splenomegaly, family history of spherocytosis, and the presence of spherocytes on a peripheral blood smear. However, it is reported that approximately 25% of patients do not have a family history; up to 20% of cases of HS without the presence of spherocytes on peripheral blood smear, or the spherocytosis is not pronounced; moderate and mild HS may have no typical clinical manifestation or even wholly asymptomatic.
Thus, moderate and mild HS, or co-occurrence of HS and other congenital HA - such as thalassemia and enzymopathies - may be misdiagnosed if only based on clinical symptoms and spherocytes appearance on smears.(2,3,4) Although conventional osmotic fragility test has been traditionally used as a gold standard for diagnosing HS, it is labor and time-consuming. There are many other confirmatory tests for HS, such as hypertonic cryohemolysis test, sodium dodecyl sulfate-polyacrylamide gel electrophoresis, ektacytometry, flow cytometry, and gene sequencing. Although every test has its advantages, an eosin-5'-maleimide binding assay (EMA) using flow cytometry has been demonstrated in many research as the most effective method for HS detection due to its convenience in time, labor, and procedure. In recent years, EMA has been used as a gold standard for HS diagnosis instead of gene sequencing in many countries because of its high sensitivity and specificity.(5,6,7)
In a developing country such as Vietnam, HS is supposed as a "rare" disease, while Thalassemias, hemoglobinopathies, and G6PD-deficiency anemia are prevalent causes of congenital hemolytic diseases. Thalassemia affects all ethnic groups in Vietnam, with up to 13% of the population being carriers.(8) Consequently, the diagnostic indices for HS and the application of modern diagnostic tools for HS in Vietnam have not received sufficient attention to date.
In this cross-sectional study, peripheral blood smear observation was used, EMA analysis, and gene sequencing in negative-direct-antiglobulin-test (neg-DAT) HA pediatrics to evaluate the utility of flow cytometry - specifically evaluate the sensitivity, specificity, accuracy, and optimal cut-off of EMA in diagnosing HS.
METHODS
Study design and participants
A cross-sectional study was conducted at Children's Hospital 1, from December 2023 to July 2024. This is the largest and most advanced pediatric hospital in Ho Chi Minh City and southern Vietnam, with many pediatric patients diagnosed with hemolytic anemia.
All patients under 18 already classified as HS or those initially diagnosed with neg-DAT hemolytic anemia were enrolled in current study. Patients who had received blood transfusions within the past month were excluded. In addition to the patient group, 44 healthy individuals were selected as a normal control group. Healthy individuals were defined as those with normal hematological parameters, normal red cell morphology, and no significant medical family history.
Data collection
A 2 mL venous blood sample, anticoagulated with K2-EDTA, was collected from each participant and analyzed within 4 hours of collection. Clinical data, including initial diagnosis, gender, age, ethnicity, medical history, and family history, were obtained from electronic medical records. Hematological parameters were measured using the Sysmex XN 2000 automated counter, which included hemoglobin concentration (Hb), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), and reticulocyte index. A Giemsa-stained peripheral blood smear was performed for each participant. Red blood cell morphological features were graded according to ICSH recommendations, with assessments carried out independently and in parallel by two experienced research fellows to ensure accuracy and objectivity.(9,10)
All patients were evaluated for level of skeletal protein deficiency to detect HS by EMA. Results were expressed as % decreased MFI (% mean fluorescent intensity decreased on red blood cells). A high % decreased MFI indicates the red cell membrane protein deficiency that leads to HS. The comparison of % decreased MFI between the patient and control groups allows us to distinguish HS patients from healthy individuals and non-HS patients (other types of neg-DAT HA). Blood samples were stored at 4 0C, and EMA was conducted within 48 hours following blood collection. Control samples from healthy individuals were collected, transported, stored, and analyzed simultaneously, following the same procedures as those used for patient samples.
The diagnosis of HS was based on a comprehensive evaluation, including clinical manifestations, individual and family medical history, routine laboratory tests, peripheral blood smear examination, and EMA binding test results. In cases where discrepancies arose between the EMA results and other diagnostic indicators, gene sequencing was performed to confirm the accuracy of the EMA binding test.
Eosin-5'-maleimide binding assay procedure
A 50 µL red pack cell centrifuged at 400g/2mins was resuspended in 2 mL phosphate buffer saline (PBS). Then, 5 µL of 0.5 mg/mL EMA dye and 2 µL CD235a were added in 50 µL red cell suspension. The EMA dye should be stored in small aliquots at -80 0C to ensure stability. The EMA-labelled red blood cell (RBC) suspension was then incubated in the dark for 30 minutes at 2-8 0C, followed by washing three times with 2 mL PBS until the supernatant became colorless to remove all excess dye. Finally, the RBC pellet was resuspended with 500 µL PBS to get the EMA-labelled RBC suspension available for flow cytometric analysis. Flow cytometric analysis was performed on a Novocyte flow cytometer (Aligent Technology, San Diego, CA, USA) for 100 µL suspension acquisition in 1.5 minutes. When binding EMA dye, the RBC population with fluorescence emission was gated on the FSC and SSC scattergram, and MFI was determined on the FL1 channel. As recommended in many previous studies and guidelines, at least 3 normal controls should be run in every batch of patient analysis to reduce intra-assay variation. In this study, 5 healthy controls were used for each analysis batch based on the recommendation by Arora RD et al.(11)
Data analysis
Data were analyzed using STATA version 17 (StataCorp, Lakeway, TX, USA). Descriptive statistics were applied, with continuous variables presented as mean ± standard deviation (SD) and range. Comparisons of continuous variables were performed using the t-test. Shapiro-Wilk test was conducted to check the distribution of the % decreased EMA binding ratio. Sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), accuracy, and the area under the ROC curve (AUC) are key metrics used to evaluate the diagnostic value of reduced EMA binding in identifying HS. The optimal cut-off point was determined by applying the maximum Youden's index (J). A p-value of < 0.05 was considered statistically significant.
Ethical considerations
The Council of Ethics in Biomedical Research at the University of Medicine and Pharmacy at Ho Chi Minh City approved this study, on November 2023 (registry number 1175/HĐĐĐ-ĐHYD). Written informed consent was obtained from all participants.
RESULTS
General characteristics of participants
From December 2023 to July 2024, 110 volunteers participated in current study, including 20 with HS, 46 patients initially diagnosed as negative-DAT hemolytic anemia (38 with thalassemia, and 8 with unidentified causes), and 44 healthy controls, with relatively equal gender (53.0% male in the patient group and 56,8% male in the control group).
Most participants belong to the Kinh ethnicity. All volunteers in the control group showed normal red blood cell indices, no signs of hemolysis or anemia, and no abnormal feature of red cell morphology on blood smear. All patient groups showed low Hb, MCV, MCH, MCHC, high reticulocyte index, and bilirubin compared with the control group, indicating that they all had active ongoing HA during our study. All 110 eligible individuals for our study were included and thoroughly analyzed. Demographic characteristics, clinical and routine laboratory data of subgroups and healthy controls are shown in table 1.
Determination of the EMA cut-off value
Of the 20 patients diagnosed as HS, all were positive for osmotic fragility (OF) test, EMA, and gene sequencing (4 ANK1/ 4 SPTA1/ 9 SPTB/ 3 SLC4A1; 18 heterozygous/ 2 homozygous). These 20 patients belonged to 20 different families, and 11/20 had a family medical history, mother or father, or both of these cases also showed decreased mean fluorescent intensity in EMA analysis and OF. Comparison of % decreased MFI showed the difference between the HS group (74.17 ± 19.88) and the control group (15.97 ± 5.47), respectively, p< 0.001.
A ROC-curve analysis was performed to determine the optimal cut-off for EMA, the area under curve (AUC) was approximately 1, respectively. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy value, and optimal cut-off were chosen by the Youden index. Based on the highest Youden index of 0.93, the optimal cut-off for the % decreased MFI in EMA was 47.83% with a sensitivity of 93.33%, specificity of 100%, PPV of 97.3%, NPV of 100%, and accuracy of 97.3%, respectively. Thus, in current study, EMA is considered positive, and HS is determined when % decreased MFI ≥ 47.83%.
Comparison of the ability of EMA and blood smear examination in the diagnosis of HS
By using the EMA cut-off value of 47.83% for further screening HS in the remaining 46 neg-DAT HA participants (38 cases of thalassemia, 2 cases diagnosed as enzyme deficiency, and 6 cases of suspected HS), there was a noticeably high % decreased MFI in 15 cases, indicating the present of HS. Gene sequencing determined these 15 positive-EMA cases and 2 negative-EMA cases to have HS gene mutations. Of these, spherocytes only appeared on blood smear at a low degree (1+), and there was no spherocyte detection in 4/9 cases of thalassemia combined with HS (table 2).
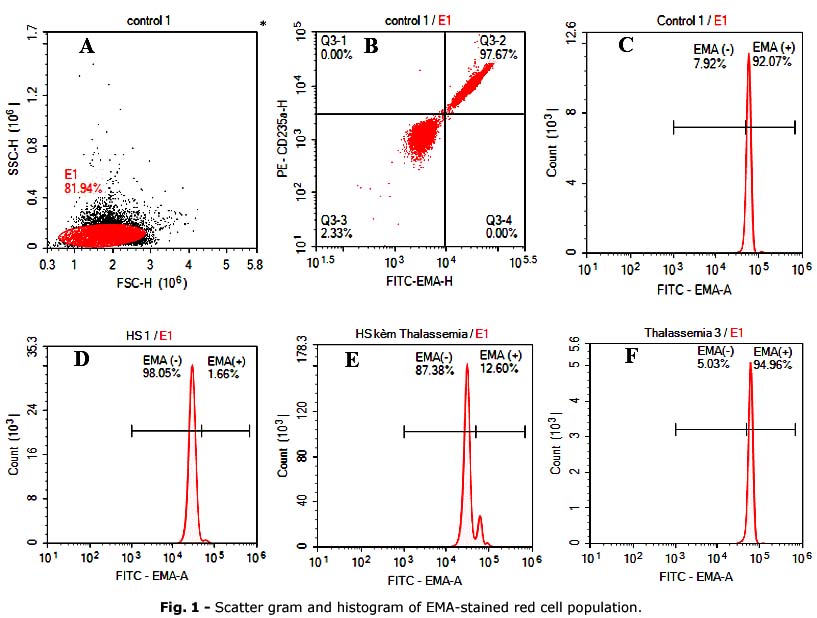
On the scattergram, the HS group had a decreased expression peak compared to the control group. The HS-combined thalassemia group has an image of two peaks that differ in the intensity of EMA expression. The thalassemia group had a reduced expression level similar to the control group (Fig. 1).
Compared to EMA, peripheral blood smear examination showed high sensitivity (82.88%). This means that this test can detect positive cases of HS well, with 29 of the 37 positive cases actually detected. However, the specificity of this test is only 33.33%, indicating that only about 1/3 of the negative cases are actually correctly identified.
The NPV is only 14.29%, that is, the ability to correctly identify cases without the disease when the result is negative. This suggests that when the peripheral smear test is negative, there is an 85.71% chance that the patient actually has the disease. In contrast, the PPV was very high (93.55%). The peripheral blood smear test has an excellent ability to detect the disease, but caution should be exercised when used in negative cases (table 3).
DISCUSSION
In the group initially diagnosed with DAT-negative hemolytic anemia, HS accounted for 36.96% (17/46) of cases. Among these, isolated HS constituted 13.04% (6/46), while HS associated with other hemolytic causes represented 23.91% (11/46). In developing Southeast Asian countries such as Vietnam, the absence of modern diagnostic tools and the belief that HS is a rare disorder have contributed to the lack of specific studies on HS patients to date. However, HS has been widely reported worldwide(12,13) with an incidence rate of about 1/2000 in Caucasians,(14) and it is the most common hereditary HA in Japan.(15)
According to Kutter D,(16) the incidence rate of HS is up to 1/150 in males and 1/800 in females when EMA is used for screening HS. In China, Wu Y et al.(7) showed that HS accounts for 31.5% of the 506 cases of hereditary hemolytic disease; also found that of the 140 children with HA admitted to the hospital, 17.9% were diagnosed with HS. Christensen RD et al.(17) used the EMA for the diagnosis of HS in 31 infants, showing that there were 11 cases of HS diagnosis, and the disease was mainly in males, accounting for 81.82% (9/11 cases).
In table 4, current results showed that the HS group had a decrease in MFI compared to the non-HS group (normal control and thalassemia). This is similar to many studies around the world. Current cut-off was higher than Glenthøj A et al.(18) (43.6%) and lower than Park SH et al.(19) (89.4%). This may be related to racial factors and patient groups in the study subjects. EMA is based on the association between EMA and band 3, in which the HS gene changes according to race, thereby influencing the expression when performing EMA.
The cut-off of Park SH et al.(19) is higher than current results because the study determined the cut-off compared to other anemia diseases such as iron deficiency anemia, chronic anemia, and autoimmune HA. Cut-off in current research was at 47.83%, with a sensitivity of 93.93% and a specificity of 100%, resulting in an overall accuracy of 97.30%. Determining the cut-off higher than other studies may reflect efforts to ensure that no cases are misdiagnosed as false negatives (table 4).
By analyzing 110 volunteers, all patients diagnosed with HS were confirmed through both EMA and gene sequencing. EMA had an impressive sensitivity of 93.93%, specificity of 100%, and accuracy of 97.3%, with the optimal cut-off determined using the Youden index. This high diagnostic performance makes EMA a superior method for screening HS compared to the peripheral blood smear, which had a sensitivity of 82.88% but a much lower specificity of 33.33%. The low specificity of blood smears indicates that a considerable proportion of negative cases may be missed, highlighting the limitations of this traditional diagnostic tool in detecting HS. The ROC curve analysis also demonstrated the robust discriminatory power of EMA, with an AUC of approximately 1, indicating near-perfect classification ability. This further justifies using EMA as a frontline diagnostic tool for HS, as it provides high sensitivity and specificity in various clinical contexts. By detecting even mild decreases in MFI, EMA can identify cases that may go undetected by routine methods, as seen in our study where some patients with Thalassemia and HS had shallow degrees of spherocytosis on blood smears yet were positive by EMA and gene sequencing.
On the other hand, the relatively low NPV of blood smears (14.29%) suggests that a negative smear result should be interpreted with caution. The high probability (over 80%) that a patient with a negative blood smear still has HS or another hemolytic condition makes the smear test an unreliable tool for ruling out HS. This is particularly concerning in a clinical setting where accurate diagnosis is crucial for timely treatment. Thus, relying solely on blood smears could lead to underdiagnosis of HS, especially in cases where spherocytes are not prominent.
Current results demonstrates that the EMA test offers superior diagnostic accuracy over peripheral blood smears for diagnosing HS. EMA's high sensitivity, specificity, and positive predictive value make it a valuable tool for screening HS in both straightforward and complex cases, such as those with coexisting hemolytic disorders. While blood smear examination remains useful, its limitations, particularly in terms of specificity and NPV, suggest that it should not be relied upon as the sole diagnostic tool. Instead, when available, a combination of tests, including EMA and genetic sequencing, should be used to ensure accurate diagnosis and appropriate clinical management of HS.
Acknowledgments
We are grateful to our participants, who kindly agreed to use their information for science and education. We are incredibly thankful to The Administrators of University of Medicine and Pharmacy at Ho Chi Minh City for supporting and funding this study. We also thank our Children's Hospital 1 colleagues for their excellent assistance.
BIBLIOGRAPHIC REFERENCES
1. Wu C, Xiong T, Xu Z, Zhan C, Chen F, Ye Y, et al. Preliminary Study on the Clinical and Genetic Characteristics of Hereditary Spherocytosis in 15 Chinese Children [Internet]. Frontiers in Genetics. 2021;12. DOI: 10.3389/fgene.2021.652376
2. Asten I, Wit H, Oirschot B, Wijk R, Vries T. Hereditary spherocytosis without pronounced spherocytes on the peripheral blood smear [Internet]. International Journal of Laboratory Hematology. 2023; 45(1):6-8. DOI: 10.1111/ijlh.13976
3. Bello A. Hereditary Spherocytosis Misdiagnosed as Glucose-6-Phosphate Dehydrogenase Deficiency [Internet]. In: Tohid H, Baratta LG, Maibach H, editors. The Misdiagnosis Casebook in Clinical Medicine: A Case-Based Guide. Cham: Springer International Publishing; 2023. p. 275-82. DOI: 10.1007/978-3-031-28296-6_39
4. Sridevi HB. Combined Hereditary Spherocytosis and β-thalassemia trait: A Rare Co-existence [Internet]. Journal of Clinical and Diagnostic Research. 2018; 12(1):9-11. DOI: 10.7860/JCDR/2018/31302.11072
5. Alvarez Flores MB, Quintero V, Bravo A, Sevilla J, Huerta J, Pacheco S, et al. Diagnosis of hereditary spherocytosis by flow cytometry in paediatric patients. Multicentric study [Internet]. Clinica Chimica Acta. 2019; 493:S597. DOI: 10.1016/j.cca.2019.03.1252
6. Chueh HW, Hwang SM, Shim YJ, Lee JM, Park HS, Lee JH, et al. Korean clinical practice guidelines for the diagnosis of hereditary hemolytic anemia [Internet]. Blood Res. 2022; 57(2):86-94. DOI: 10.5045/br.2022.2021224
7. Wu Y, Liao L, Lin F. The diagnostic protocol for hereditary spherocytosis-2021 update [Internet]. JClin LabAnal. 2021; 35(12):e24034. DOI: 10.1002/jcla.24034
8. Tran DC, Dang AL, Hoang TNL, Nguyen CT, Le TMP, Dinh TNM, et al. Prevalence of Thalassemia in the Vietnamese Population and Building a Clinical Decision Support System for Prenatal Screening for Thalassemia [Internet]. Mediterr J Hematol Infect Dis. 2023; 15(1):e2023026. DOI: 10.4084/mjhid.2023.026
9. Palmer L, Briggs C, McFadden S, Zini G, Burthem J, Rozenberg G, et al. ICSH recommendations for the standardization of nomenclature and grading of peripheral blood cell morphological features [Internet]. Int J Lab Hematol. 2015; 37(3):287-303. DOI: 10.1111/ijlh.12327
10. Chase ML, Drews R, Zumberg MS, Ellis LR, Reid EG, Gerds AT, et al. Consensus recommendations on peripheral blood smear review: defining curricular standards and fellow competency [Internet]. Blood Advances. 2023; 7(13):3244-52. DOI: 10.1182/bloodadvances.2023009843
11. Arora RD, Dass J, Maydeo S, Arya V, Radhakrishnan N, Sachdeva A, et al. Flow cytometric osmotic fragility test and eosin-5'-maleimide dye-binding tests are better than conventional osmotic fragility tests for the diagnosis of hereditary spherocytosis [Internet]. Int J Lab Hematol. 2018; 40(3):335-42. DOI: 10.1111/ijlh.12794
12. Liu Y, Zheng J, Song L, Fang Y, Sun C, Li N, et al. A novel SPTB gene mutation in neonatal hereditary spherocytosis: A case report [Internet]. Exp Ther Med. 2020; 20(4):3253-9. DOI: 10.3892/etm.2020.9062
13. Choi HS, Choi Q, Kim JA, Im KO, Park SN, Park Y, et al. Molecular diagnosis of hereditary spherocytosis by multi-gene target sequencing in Korea: matching with osmotic fragility test and presence of spherocyte [Internet]. Orphanet J Rare Dis. 2019; 14(1):114. DOI: 10.1186/s13023-019-1070-0
14. King MJ, Garçon L, Hoyer JD, Iolascon A, Picard V, Stewart G, et al. ICSH guidelines for the laboratory diagnosis of nonimmune hereditary red cell membrane disorders [Internet]. International journal of laboratory hematology. 2015; 37(3):304-25. DOI: 10.1111/ijlh.12335
15. Yamamoto KS, Utshigisawa T, Ogura H, Aoki T, Kawakami T, Ohga S, et al. Clinical and genetic diagnosis of thirteen Japanese patients with hereditary spherocytosis [Internet]. Human Genome Variation. 2022; 9(1):1. DOI: 10.1038/s41439-021-00179-1
16. Kutter D. Hereditary spherocytosis is more frequent than expected: what to tell the patient? [Internet]. Bulletin de la Societe des Sciences Medicales du Grand-duche de Luxembourg. 2005; 12(1):7-22. DOI: 10.1002/jcla.24034
17. Christensen RD, Agarwal AM, Nussenzveig RH, Heikal N, Liew MA, Yaish HM. Evaluating eosin-5-maleimide binding as a diagnostic test for hereditary spherocytosis in newborn infants [Internet]. J Perinatol. 2015; 35(5):357-61. DOI: 10.1002/jcla.24034
18. Glenthøj A, Brieghel C, Nardo-Marino A, van Wijk R, Birgens H, Petersen J. Facilitating EMA binding test performance using fluorescent beads combined with next-generation sequencing [Internet]. EJHaem. 2021; 2(4):716-28. DOI: 10.1002/jha2.277
19. Park SH, Park C-J, Lee B-R, Kim YJ, Cho Y-U, Jang S, et al. Screening for hereditary spherocytosis: EMA binding test and flow cytometric osmotic fragility test are recommended, but cryohemolysis test is not recommended [Internet]. Blood. 2013; 122(21):3425. DOI: 10.1182/blood.V122.21.3425.3425
Conflicts of interests
No potential conflict of interest relevant to this article was reported.
Financial information
The University of Medicine and Pharmacy at Ho Chi Minh City funded this research under contract number 65/2024/ HĐ-ĐHYD, Dated 15/ 04/ 2024.
Authors' contributions
Conceptualization: Hien Thanh Dao.
Data curation:
Tuyet Thi Bach Tran, Hien Thanh Dao, Anh Thi Mai Nguyen.
Formal analysis: Triet Hy Van, Hien Thanh Dao, Anh Thi Mai Nguyen.
Research:
Tuyet Thi Bach Tran, Hien Thanh Dao, Triet Hy Van, Anh Thi Mai Nguyen.
Methodology:
Tuyet Thi Bach Tran, Hien Thanh Dao, Triet Hy Van, Anh Thi Mai Nguyen.
Supervision: Dat Quoc Ngo, Anh Thi Mai Nguyen.
Validation: Dat Quoc Ngo, Anh Thi Mai Nguyen.
Writing - original draft: Hien Thanh Dao, Triet Hy Van.
Writing - review and editing: Triet Hy Van.
Data availability statement
This research data is confidential according to the applicable confidentiality agreements and regulations and, therefore, cannot be publicly displayed or shared. The data are securely stored at the Integrated Planning Department at Children's Hospital 1. Access to these data requires proper authorization. If you have any questions or need further information, please get in touch with Triet Hy Van at vanhytriet@ump.edu.vn