Clinical Practice Article
Outcomes of treating unstable thoracolumbar fractures without spinal cord injury using percutaneous pedicle screw fixation
Resultados del tratamiento de fracturas toracolumbares inestables sin lesión de la médula espinal mediante fijación percutánea de tornillos transpediculares
Dinh Cong Ham1
https://orcid.org/0009-0007-2799-8439
Pham
Vo Ky2,3
https://orcid.org/0009-0007-8462-5639
Dang
Van Thich1
https://orcid.org/0009-0000-5245-8732
Nguyen
Trung Hau1
https://orcid.org/0009-0005-2766-6413
Nguyen
Huu Tai4
https://orcid.org/0009-0002-8875-161X
Ha
Thoai Ky4
https://orcid.org/0009-0000-0673-1945
Vo
Le Thanh Phuc4
https://orcid.org/0009-0006-9875-1014
Nguyen
Duy Linh4*
https://orcid.org/0000-0001-8283-9237
1121
Military Hospital. Department of Neurosurgery. Can Tho, Vietnam.
2Kien
Giang General Hospital. Department of Neurosurgery. Kien Giang, Vietnam.
3Cuu
Long University. Department of Health Sciences. Vinh Long, Vietnam.
4Can
Tho University of Medicine and Pharmacy. Department of Surgery. Can Tho, Vietnam.
*Author for correspondence. Email: ndlinh@ctump.edu.vn
Background:
Unstable thoracolumbar fractures can lead to pain and limited mobility.
Minimally invasive spinal surgery, particularly percutaneous pedicle screw fixation,
has shown promise in restoring spinal stability with reduced soft tissue damage
and faster recovery.
Objectives: To evaluate the outcomes of treating thoracolumbar fractures
via percutaneous pedicle screw fixation.
Methods: A retrospective case series was conducted on 32 patients with
unstable thoracolumbar fractures (T11-L2) without spinal cord injury. Exclusion
criteria included neurological deficits, pathological fractures, or incomplete
records. Operative time, blood loss, complications, VAS scores, Cobb angles,
and Macnab criteria were assessed. Surgery was performed under fluoroscopic
guidance via small incisions without muscle detachment.
Results:
Among the 32 patients, 20 were males (62.5%) and 12 were females (37.5%),
with a mean age of 46.2 ± 11.1 years. The average preoperative kyphotic angle
was 14.4°±4.3°, which decreased to 8.1°±3.6° postoperatively (t value= 15.153;
p<0.001). The mean pain score, measured by the visual analog scale (VAS),
was 6.8±1.5 preoperatively and decreased to 1.2±0.7 at six months postoperatively
(p<0.05). Intraoperative complications included one case of lateral pedicle
wall injury. Postoperative complications included one case of superficial infection
at the surgical site. The Macnab criteria were rated as excellent in 31 patients
(96.9%) and good in 1 patient (3.1%).
Conclusions:
Percutaneous pedicle screw fixation is a safe and effective method for treating
unstable thoracolumbar fractures without spinal cord neurological impairment.
Keywords: minimally invasive surgery; percutaneous pedicle screw fixation; thoracolumbar fracture.
Antecedentes:
En las fracturas toracolumbares inestables (FTI), la cirugía espinal mínimamente
invasiva, en particular la fijación percutánea con tornillos transpediculares,
demuestra ser prometedora para restaurar la estabilidad espinal, con menor daño
a los tejidos blandos y recuperación más rápida.
Objetivos: Evaluar los resultados del tratamiento de FTI mediante fijación
percutánea de tornillos transpediculares.
Métodos: Serie de casos retrospectiva de 32 pacientes con FTI (T11-L2),
sin lesión medular. Criterios de exclusión: Déficits neurológicos, fracturas
patológicas o expedientes incompletos. Se evaluó: Tiempo operatorio, pérdida
de sangre, complicaciones, puntuaciones de la escala visual analógica (EVA),
ángulos de Cobb y criterios de Macnab. La cirugía se realizó bajo guía fluoroscópica,
a través de pequeñas incisiones, sin desprendimiento muscular.
Resultados: Según sexo: 20 hombres (62,5 %) y 12 mujeres (37,5 %); edad
media 46,2 ± 11,1 años. Ángulo cifótico preoperatorio promedio: 14,4 ° ± 4,3
°, disminuyó a 8,1 ° ± 3,6 ° después de la cirugía (valor t= 15,153; p< 0,001).
Puntaje promedio de dolor (EVA): 6,8 ± 1,5 antes de la operación, disminuyó
a 1,2 ± 0,7, a los 6 meses postoperatorios (p< 0,05). Complicaciones intraoperatorias:
1 caso de lesión de pared lateral del pedículo; las postoperatorias, 1 caso
de infección superficial en sitio quirúrgico. Según criterios de Macnab: Excelente
en 31 pacientes (96,9 %) y bueno en 1 paciente (3,1 %).
Conclusiones:
La fijación percutánea de tornillos transpediculares es un método seguro
y eficaz para tratar fracturas inestables toracolumbares sin afectación neurológica
de la médula espinal.
Palabras clave: cirugía mínimamente invasiva; fijación percutánea de tornillos transpediculares; fractura toracolumbar.
Received: 09/12/2024
Approved:
06/06/2025
INTRODUCTION
Spinal trauma is a common surgical emergency, accounting for approximately 6% of all trauma cases. Among these, thoracolumbar spinal injuries (T11-L2) are the most common, accounting for approximately 60-70% of cases. The majority of these injuries are unstable spinal fractures without spinal cord injury, accounting for 80-85% of cases.(1) Managing thoracolumbar fractures is a significant challenge that requires close multidisciplinary collaboration to achieve optimal outcomes.
Traditional surgical methods for treating thoracolumbar fractures have notable limitations, including long incisions, extensive muscle dissection, and transection, which result in significant soft tissue damage, increased intraoperative blood loss, a greater risk of infection, and prolonged hospital stays. Furthermore, damage to the paraspinal muscles during surgery can lead to subsequent muscle degeneration and atrophy.(2,3)
In recent years, minimally invasive surgery has emerged as a groundbreaking solution.(4,5,6,7) Specifically, compared with traditional open surgery, percutaneous pedicle screw fixation has several advantages, including minimal soft tissue damage, reduced blood loss, fewer postoperative complications, and shorter recovery times.(8,9)
To evaluate the effectiveness of this minimally invasive technique in our region, we conducted a study on the outcomes of treating thoracolumbar fractures via percutaneous pedicle screw fixation.
METHODS
Study design
This retrospective descriptive study included 32 patients with unstable thoracolumbar fractures without spinal cord neurological deficits.
Subjects
The study subjects included patients diagnosed with thoracolumbar spinal fractures who underwent percutaneous pedicle screw fixation at 121 Military Hospital in Can Tho city, Vietnam from July 2022 to October 2023.
Inclusion criteria
Exclusion criteria
Variables
The study assessed several key variables, including age and sex for each participant. Clinical and imaging features, including the cause of injury, VAS pain score, fracture location, and classification of thoracolumbar vertebral fractures, were evaluated. Surgical outcomes were assessed by the accuracy of screw placement, graded according to the Heary classification (grades I-V):(10) Grade I indicates the screw is entirely situated within the pedicle; Grade II refers to the screw perforating the lateral pedicle wall, though its tip remains fully contained within the vertebral body; Grade III occurs when the screw tip extends through the anterior or lateral aspect of the vertebral body; Grade IV denotes the screw breaching the medial or inferior wall of the pedicle; and Grade V describes the screw violating the pedicle or vertebral body, posing a direct threat to the spinal cord, nerve roots, or great vessels, and thus necessitating immediate corrective surgery. Operative time, intraoperative blood loss, hospital stay duration, complications, radiological outcomes (Cobb angle), and VAS scores were recorded and analyzed. Both intraoperative and postoperative complications were documented, alongside VAS pain scores at 1, 3, and 6 months. Finally, functional outcomes were evaluated using Macnab's criteria at the 6-month postoperative mark.
Percutaneous pedicle screw fixation procedure
Step 1: Patient position: All procedures were performed under general anesthesia. The patient was positioned prone on the radiolucent table, and C-arm fluoroscopy was used to confirm clear visualization of the fractured vertebra and pedicle. The spinous process was centered between the pedicles, and the endplates of the vertebral body to be instrumented were parallel to one another.
Step 2: Needle Insertion: The skin incision was made approximately 1-1.5cm lateral to the outer border of the pedicle or at the tip of the transverse process. Under C-arm fluoroscopic guidance, a Jamshidi needle was advanced through the incision, targeting the outer edge of the pedicle at the 3:00 position on the right side and 9:00 on the left. The needle was inserted to a depth of 20-25 mm within the pedicle, with continuous fluoroscopic confirmation to ensure that it remained lateral to the medial pedicle wall. Proper trajectory and depth were confirmed in both anteroposterior and lateral views before proceeding with guidewire insertion (Fig.1A).
Step 3: Screwinsertion, reduction, and stabilization: Confirm the screw trajectory via the C-arm in the lateral view (verify that the needle reaches the medial pedicle edge in the anteroposterior view and the middle of the pedicle body in the lateral view). The needle was advanced into the vertebral body (approximately halfway along the posterior vertebral body). A guidewire was inserted through the needle, and the Jamshidi needle was removed. Sequential dilators were used to gently separate the soft tissue, beginning with 5.0 mm and 6.0 mm dilators, followed by a 9.3 mm large dilator. A working cannula was then inserted to maintain the pathway for screw insertion. Pedicle preparation was performed using a cannulated tap with a diameter of 4.5 mm to 5.5 mm depending on the screw size. In cases of particularly hard bone, the self-drilling tap option was employed. Fluoroscopy was used to confirm guidewire and Tap positions throughout. Screw length was estimated by referencing the depth markings on the tap against the rim of the large dilator. After tapping, the dilator was removed while keeping the guidewire in place. Prior to screw insertion, the Screw Extenders were assembled by inserting the Inner Sleeve into the Extender and compressing the flexible tabs. The complete Extender-Screw assembly was advanced over the guidewire and into the pedicle. If resistance was encountered, the assembly was withdrawn, and the pedicle was retapped using a tap of the same diameter as the selected screw. Cannulated pedicle screws with a shaft length of 40-45 mm and diameters of 5.5-6.0 mm were used. The multiaxial heads allowed rod connection through the percutaneous system. Care was taken not to over-insert the screw, as excessive force on the multiaxial head could compromise its mobility, complicating rod placement in subsequent steps. Once the screw was fully seated, the guidewire was removed (Fig.1B).
Data analysis
Data were processed and analyzed via SPSS 23.0 software. A paired comparison method was used to evaluate the effectiveness of the intervention before and after treatment in the same subjects. For pain level assessment, the Cobb angle before and after surgery (quantitative variables), a t test was applied if the data followed a normal distribution; the Wilcoxon test was used if the distribution was not normal. A p value of < 0.05 was considered statistically significant.
Ethical considerations
The study was conducted following approval from the Ethics Council in Biomedical Research, Can Tho University of Medicine and Pharmacy, under approval number 22.102.HV-ÐHYDCT and was authorized by the Directorate of 121 Military Hospital. The study was in line with the Declaration of Helsinki. Written informed consent was obtained from all participants after full explanation.
RESULTS
General characteristics
There was a greater proportion of males (20 patients; 62.5%) and 12 females (37.5%). The average age of the patients was 46.2 ± 11.1 years, with the youngest patient being 20 years old and the oldest being 70 years old. The majority of patients were in the working-age group (20-60 years), with 27 cases accounting for 84.4%. The largest subgroup was 41-50 years old, with 11 cases (34.4%).
Clinical characteristics and imaging findings of thoracolumbar spine fractures
Fall from height was a common type of accident associated with thoracolumbar fracture, with 14 cases, accounting for 43.8% of all accidents. Traffic accidents and falls during daily activities have similar frequencies, with 9 cases each, representing 28.1%. The preoperative average VAS score was 6.8 ± 1.5. Most patients experienced severe back pain (VAS score 7-8) in 16 patients, accounting for 50.0% of all patients. Moderate pain (VAS score ranging from 4-6) was reported in 11 patients (34.4%). Worst pain (VAS score 9-10) was observed in 5 patients (15.6%). The most common level of injury was L1, with 16 patients (50.0%). Burst fractures (A3, A4) accounted for the highest proportion, with 29 cases (90.6%) (table 1).
Outcomes
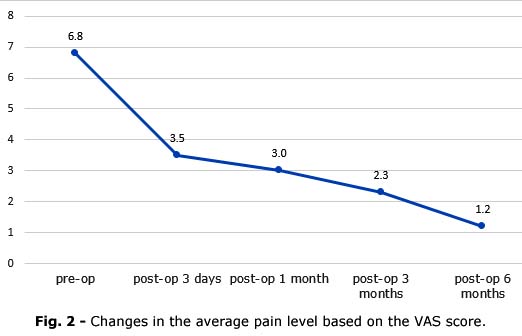
There was a significant improvement in the average pain level based on the VAS score after surgery. Three days after surgery, the average pain score decreased to 3.5 ± 1.2, compared to 6.8 ± 1.5 before surgery, and further decreased to 1.2 ± 0.8 at the 6-month follow-up (Fig. 2). The differences in pain levels across these time points were statistically significant (pair-sample t test, p< 0.05).
The mean surgical duration was 84.2 ± 22.8 minutes, ranging from 70-150 minutes. The mean blood loss was 46.1 ± 39.6 ml, ranging from a minimum of 10 ml to a maximum of 150 ml. The average duration from surgery to discharge was 7.1 ± 6.7 days, with the shortest duration being 5 days and the longest duration being 13 days. The accuracy of pedicle screw placement, according to Heary's criteria, was 96.9%, with one case in which the screw was placed on the lateral wall of the pedicle without causing neural damage (3.1%). The mean Cobb angle before surgery was 14.3 ± 4.3, whereas the average Cobb angle after surgery was 8.1 ± 3.6. A significant difference (p< 0.001) was observed in the degree of spinal alignment correction during surgery (table 2). An illustrative case showing radiographic changes in Cobb angle before and after correction is presented in Fig. 3.
DISCUSSION
General characteristics
In the series, 32 patients, 20 males (62.5%) and 12 females (37.5%) with thoracolumbar spine fractures, underwent percutaneous pedicle screw fixation. The average age of the patients was 46.2 ± 11.1 years, with the youngest patient being 20 years old and the oldest being 70 years old. The majority of patients were in the working-age group (20 - 60 years), with 27 cases accounting for 84.4%. The largest subgroup was 41-50 years old, with 11 cases (34.4%). This findings are consistent with those of other studies, such as those by McAnany SJ et al.(11) and Hong SH et al.(12)
Clinical features and imaging of thoracolumbar spinal fractures
Clinical features
Similarities were found when comparing the causes of injury in the current study with those reported by other authors, both domestic and international. Vanek P et al.(13) conducted a study on 19 cases of percutaneous pedicle screw fixation and reported that falls from a height were the most common cause, accounting for 10 cases. In such falls, the mechanism of injury is often compressive along the longitudinal axis, with the majority of injuries being mild and causing vertebral body collapse. This type of injury is typically suitable for percutaneous pedicle screw fixation.
Preoperatively, the average VAS pain score was 6.8 ± 1.5, with most patients experienced severe back pain (VAS score 7-8) in 16 patients, accounting for 50.0% of all patients. Moderate pain (VAS score 4-6) was reported in 11 patients (34.4%), whereas worst pain (VAS score 9-10) was observed in 5 patients (15.6%). For patients with spinal fractures without neurological deficits, pain is often a hallmark symptom, prompting imaging studies to assess the injury and guide treatment.
Imaging characteristics
Current study revealed that fractures were most common at the L1 vertebra in 16 patients (50.0%). These results are consistent with those of previous studies, such as those by Fitschen-Oestern S et al.(14) and Hong SH et al.(12), who reported that L1 and T12 were the most commonly affected levels. The thoracolumbar junction is particularly vulnerable to injury because it is located at the transition point between the rigid thoracic spine and the more mobile lumbar spine. Additionally, T11 and T12 are free-floating ribs that do not attach directly to the sternum, reducing stability. The facet joints of the lumbar spine are oriented in the sagittal plane, in contrast to the frontal plane of the thoracic spine.
With respect to the AO thoracolumbar injury classification, burst fractures (A3, A4) accounted for the greatest proportion, with 29 cases (90.6%), which is in line with the findings of Fitschen-Oestern S et al.(14), where A3 fractures were the most common.
Surgical Outcomes
There was a significant improvement in the average pain level according to the VAS score, with a postoperative score of 3.5 ± 1.2 on the third day compared with 6.8 ± 1.5 before surgery and 1.2 ± 0.8 at 6 months after discharge. The differences in average pain levels at these time points were statistically significant, with p< 0.05. The percutaneous pedicle screw fixation method is a minimally invasive approach that helps reduce pain and accelerate recovery, with a low complication rate of 1/32 patients (3.1%).
In this study, the average amount of blood loss during surgery was minimal. Elenany SA et al.(2) reported an average blood loss of 174 ml. Afolabi A et al.(15) reported 136 ml versus 606 ml in open surgery. The minimally invasive percutaneous pedicle screw method with a small incision causes minimal tissue damage and helps reduce blood loss.
The average Cobb angle in current study group before surgery was 14.3 ° ± 4.3 °, and after surgery, the average Cobb angle was 8.1 ° ± 3.6 °. This change was statistically significant at p< 0.001. Elenany SA et al.(2) reported that the correction angle was 3.3 0. Previous studies have shown that, compared with open surgery, spinal alignment correction is not a major advantage of percutaneous screw fixation. For patients with significant kyphosis, open surgery should be considered to achieve appropriate alignment.(16,17)
The study evaluating the outcomes of percutaneous pedicle screw fixation for treating unstable thoracolumbar fractures without spinal cord injury revealed substantial improvements in both spinal alignment and pain management. Specifically, the kyphotic angle decreased from 14.4° to 8.1°, and the VAS pain score improved significantly, from 6.8 to 1.2, within six months postoperatively. These results align closely with those from other studies that have evaluated similar surgical approaches.(6,18)
Esposito F et al.(17) reported reduced hospital stays, with patients who underwent minimally invasive surgery remaining an average of 1.5 days less than those who underwent open surgery. In terms of complications, minimally invasive surgery was associated with a reduction in infection rates and other adverse events. These findings mirror current study, where we observed a low complication rate-one case of superficial infection and one case of lateral pedicle wall injury-further supporting the safety and efficacy of the minimally invasive approach.
In a prospective study by Elenany SA et al.(2), the role of percutaneous fixation was assessed for thoracolumbar fractures. They reported that this technique not only provided excellent fracture stability but also resulted in significant pain reduction, with patients showing a 70% decrease in VAS score postoperatively. Similarly, current study revealed a reduction in the VAS score from 6.8 to 1.2, reflecting comparable pain management outcomes. Additionally, Elenany SA et al.(2) reported that patients experienced fewer complications, which aligns with the relatively low complication rate observed in current study.
Afolabi A et al.(15) also compared percutaneous fixation with open surgery for treating thoracolumbar fractures and reported that the minimally invasive group had a significantly shorter recovery time. In their study, 85% of the minimally invasive patients returned to full activity within 3 months, whereas only 50% of those who underwent open surgery returned. The results of this study demonstrate that percutaneous pedicle screw fixation effectively reduces the kyphotic angle and improves postoperative pain in patients with unstable thoracolumbar fractures without neurological deficits. Notably, the minimally invasive approach resulted in reduced blood loss and shorter operative times, supporting its feasibility in selected cases. Compared to open fixation techniques, this method preserved paraspinal musculature and minimized soft tissue damage.(16,17) The high success rate and low complication profile in our series may be attributed to meticulous fluoroscopic guidance and standardized screw placement techniques.
Percutaneous pedicle screw fixation with small incision and the use of a dilator system to separate soft tissues and lumbar muscles, avoiding extensive dissection and electrocautery, such as in open surgery, is very useful in reducing postoperative pain, minimizing blood loss during surgery, shortening the hospital stay, reducing complications, and improving patient recovery. Therefore, percutaneous pedicle screw fixation is considered a safe, valid, and effective treatment method for patients with thoracolumbar spinal fractures without neurological deficits.(8,9,19)
This study has several limitations. First, the small sample size and single-center design limit the generalizability of the results to broader populations. Second, no control group for comparison restricts strong conclusions about the superiority of percutaneous pedicle screw fixation over open surgery. Lastly, short follow-up period of 6 months may underestimate long-term complications or instrument-related issues.
Percutaneous pedicle screw fixation is a safe and effective treatment method for unstable thoracolumbar spine fractures without neurological deficits. It has high efficacy and low complication rates. There was a significant improvement in the VAS score and Cobb angle postoperatively.
Acknowledgements
We sincerely acknowledge the invaluable support provided by Can Tho University of Medicine and Pharmacy and 121 Military Hospital during the implementation of this study.
BIBLIOGRAPHIC REFERENCES
1. Whitney E, Alastra AJ. Vertebral Fracture [Internet]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 [access: 30/11/2024]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK547673/
2. Elenany SA, Alkosha HA, Ibrahiem MS. Role of minimally invasive percutaneous fixation in thoracolumbar fractures: a prospective study [Internet]. Egypt J Neurosurg. 2019 Dec 4;34(1):40. DOI: 10.1186/s41984-019-0063-6
3. Tu P, Yan C chao, Hao J xue, Cao S, Jiang C. Effect of percutaneous minimally invasive pedicle screw internal fixation in the treatment of thoracolumbar vertebral fractures and its impact on quality of life [Internet]. Pak J Med Sci. 2022;38(1):100-5. DOI:10.12669/pjms.38.1.4329
4. Tran C, Nguyen L, Nguyen H, Tran V, Ha M. Minimally invasive laminectomy treated thoracic spinal cord compression caused by ossification flavum ligament: first case report in Mekong Delta, Vietnam and Literature review [Internet]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023;58:757-63. Available from: https://www.zhebyhk-periodicals-cn.net/article/minimally-invasive-laminectomy-treated-thoracic-spinal-cord-compression-caused-by-ossification-flavum-ligament-first-case-report-in-mekong-delta-vietnam-and-literature-review
5. Neeley OJ, Kafka B, Tecle NE, Shi C, El Ahmadieh TY, Sagoo NS, et al. Percutaneous screw fixation versus open fusion for the treatment of traumatic thoracolumbar fractures: A retrospective case series of 185 Patients with a single-level spinal column injury [Internet]. J Clin Neurosci. 2022;101:47-51. DOI: 10.1016/j.jocn.2022.04.045
6. Lu J, Chen Y, Hu M, Sun C. Systematic review and meta-analysis of the effect of using percutaneous pedicle screw internal fixation for thoracolumbar fractures [Internet]. Ann Palliat Med. 2022;11(1):25059-259. DOI: 10.21037/apm-21-3736
7. Kocis J, Kelbl M, Kocis T, Návrat T. Percutaneous versus open pedicle screw fixation for treatment of type A thoracolumbar fractures [Internet]. Eur J Trauma Emerg Surg Off Publ Eur Trauma Soc. 2020;46(1):147-52. DOI: 10.1007/s00068-018-0998-4
8. Oh T, Scheer JK, Fakurnejad S, Dahdaleh NS, Smith ZA. Minimally invasive spinal surgery for the treatment of traumatic thoracolumbar burst fractures [Internet]. J Clin Neurosci. 2015;22(1):42-7. DOI: 10.1016/j.jocn.2014.05.030
9. Yang M, Zhao Q, Hao D, Chang Z, Liu S, Yin X. Comparison of clinical results between novel percutaneous pedicle screw and traditional open pedicle screw fixation for thoracolumbar fractures without neurological deficit [Internet]. Int Orthop. 2019;43(7):1749-54. DOI: 10.1007/s00264-018-4012-x
10. Heary RF, Bono CM, Black M. Thoracic pedicle screws: postoperative computerized tomography scanning assessment [Internet]. J Neurosurg. 2004;100(4 Suppl Spine):325-31. DOI: 10.3171/spi.2004.100.4.0325
11. McAnany SJ, Overley SC, Kim JS, Baird EO, Qureshi SA, Anderson PA. Open versus Minimally Invasive Fixation Techniques for Thoracolumbar Trauma: A Meta-Analysis [Internet]. Glob Spine J. 2016;6(2):186-94. DOI: 10.1055/s-0035-1554777
12. Hong SH, Suh SP, Yeom J, Kim JY, Lee SG, Han JW. Minimally Invasive Spine Surgery versus Open Posterior Instrumentation Surgery for Unstable Thoracolumbar Burst Fracture [Internet]. Asian Spine J. 2021;15(6):761-8. DOI: 10.31616/asj.2020.0572
13. Vanek P, Bradac O, Konopkova R, Lacy P de, Lacman J, Benes V. Treatment of thoracolumbar trauma by short-segment percutaneous transpedicular screw instrumentation: prospective comparative study with a minimum 2-year follow-up [Internet]. J Neurosurg Spine. 2014;20(2):150-6. DOI: 10.3171/2013.11.SPINE13479
14. Fitschen-Oestern S, Scheuerlein F, Weuster M, Klueter T, Menzdorf L, Varoga D, et al. Reduction and retention of thoracolumbar fractures by minimally invasive stabilisation versus open posterior instrumentation [Internet]. Injury. 2015;46 (Suppl 4):S63-70. DOI: 10.1016/S0020-1383(15)30020-6
15. Afolabi A, Weir TB, Usmani MF, Camacho JE, Bruckner JJ, Gopinath R, et al. Comparison of percutaneous minimally invasive versus open posterior spine surgery for fixation of thoracolumbar fractures: A retrospective matched cohort analysis [Internet]. J Orthop. 2020;18:185-90. DOI: 10.1016/j.jor.2019.11.047
16. Defino HLA, Costa HRT, Nunes AA, Nogueira Barbosa M, Romero V. Open versus minimally invasive percutaneous surgery for surgical treatment of thoracolumbar spine fractures- a multicenter randomized controlled trial: study protocol [Internet]. BMC Musculoskelet Disord. 2019;20(1):397. DOI: 10.1186/s12891-019-2763-1
17. Esposito F, Bove I, Vitulli F, Bocchino A, Barbanera A, Nape S, et al. Outcome Measures of Open versus Minimally Invasive Surgery for Thoracolumbar Spinal Traumatic Fractures: A Systematic Review and Meta-Analysis [Internet]. J Clin Med. 2024;13(18):5558. DOI: 10.3390/jcm13185558
18. Tinelli M, Töpfer F, Kreinest M, Matschke S, Grützner PA, Suda AJ. Minimally invasive reduction and percutaneous posterior fixation of one-level traumatic thoraco-lumbar and lumbar spine fractures [Internet]. Eur J Orthop Surg Traumatol. 2018;28(8):1581-7. DOI: 10.1007/s00590-018-2224-9
19. Pannu CD, Farooque K, Sharma V, Singal D. Minimally invasive spine surgeries for treatment of thoracolumbar fractures of spine: A systematic review [Internet]. J Clin Orthop Trauma. 2019;10:S147-55. DOI: 10.1007/s00590-018-2224-9
Conflicts of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors declare that no grants were involved in this work.
Authorship contribution
Conceptualization: Pham Vo Ky, Dinh Cong Ham, Dang Van Thich, Nguyen Duy
Linh.
Data
curation: Dinh Cong Ham, Dang Van Thich, Nguyen Trung Hau.
Formal
analysis: Dinh Cong Ham, Nguyen Duy Linh, Ha Thoai Ky, Vo Le Thanh Phuc.
Investigation:
Dinh Cong Ham, Nguyen Duy Linh, Ha Thoai Ky, Vo Le Thanh Phuc.
Research:
Dinh Cong Ham, Pham Vo Ky, Nguyen Duy Linh, Nguyen Huu Tai, Vo Le Thanh
Phuc.
Resources:
Dang Van Thich, Nguyen Trung Hau.
Software:
Dinh Cong Ham, Nguyen Duy Linh.
Methodology:
Dinh Cong Ham, Pham Vo Ky, Nguyen Duy Linh.
Project
administration: Dinh Cong Ham, Pham Vo Ky.
Supervision:
Pham Vo Ky, Dang Van Thich.
Validation
: Dinh Cong Ham, Nguyen Duy Linh, Ha Thoai Ky.
Visualization:
Dinh Cong Ham, Nguyen Duy Linh.
Writing
- original draft: Dinh Cong Ham, Nguyen Duy Linh, Ha Thoai Ky, Vo Le Thanh
Phuc.
Writing
- Review & editing: Dinh Cong Ham, Pham Vo Ky, Nguyen Duy Linh.
Data availability statement
All data underlying the results are available as part of the article and no additional source data are required.