Case Presentation
Sinusal fungal ball as a consequence of long-term hydrocortisone therapy
Bola fúngica sinusal como consecuencia del tratamiento prolongado con hidrocortisona
Rony Ludeña-Yance1 https://orcid.org/0009-0003-4669-8838
Patricia Yacono-Ruiz1 https://orcid.org/0009-0006-2866-7343
Rosa Campos-Yaipen2 https://orcid.org/0009-0007-4138-2227
Pierre Mendoza-Montoya3* https://orcid.org/0000-0003-2197-7550
José Salvador-Carrillo1 https://orcid.org/0000-0001-7076-6093
1Universidad Privada San Juan Bautista. Escuela Profesional de Medicina Humana. Chincha, Perú.
2Universidad Nacional Mayor de San Marcos. Facultad de Farmacia y Bioquímica. Lima, Perú.
3Universidad Privada San Juan Bautista. Escuela Profesional de Medicina Humana. Lima Perú.
*Autor para la correspondencia. Correo electrónico: jfsc135@gmail.com
ABSTRACT
Introduction: Diagnosis of sinus fungal ball (SFB) remains a challenge in clinical practice. However, the use of corticosteroids in patients with autoimmune diseases may increase the risk of occurrence.
Objective: To report the occurrence of sinus fungal ball after long-term treatment with hydrocortisone in an autoimmune patient.
Case report: A 57-year-old patient, diagnosed with Addison's disease (AD) at age 21 and on continuous hydrocortisone therapy since then, presented to the healthcare facility. Initially, bacterial sinusitis was suspected, and he underwent multiple antibiotic courses over six months. On computed tomography, pseudopneumatization with an oval image compatible with a fungal ball was observed. Finally, SFB was removed nine months after the initial medical care. The level of causality between sinus fungal ball and hydrocortisone was "possible" and had a "moderate" severity level.
Conclusions: Healthcare professionals should consider the diagnosis of sinus fungal ball in immunocompromised patients during clinical practice and should remain alert to the possibility of fungal infections as side effects of long-term corticosteroid therapy.
Keywords: drug-related side effects and adverse reactions; fungal infection; hydrocortisone; medication errors.
RESUMEN
Introducción: El diagnóstico de bola fúngica sinusal sigue representando un desafío en la práctica clínica. No obstante, el uso de corticosteroides en pacientes con enfermedades autoinmunes puede aumentar el riesgo de su aparición.
Objetivo: Reportar la ocurrencia de bola fúngica sinusal tras un tratamiento prolongado con hidrocortisona en un paciente autoinmune.
Caso Clínico: Paciente de 57 años, diagnosticado con la enfermedad de Addison desde los 21 años y en tratamiento continuo con hidrocortisona desde entonces, acude al establecimiento de salud. Inicialmente, se sospechó sinusitis bacteriana, por lo que recibió un régimen antibiótico de 6 meses. Posteriormente, en una evaluación por tomografía computarizada, se observó una pseudoneumatización con imagen ovalada compatible con bola fúngica. Finalmente, la bola fúngica sinusal se extrajo 9 meses después de la primera atención médica. El nivel de causalidad entre la bola fúngica sinusal y la hidrocortisona se clasificó como "posible", con un nivel de gravedad "moderado".
Conclusiones: Los profesionales de la salud deben considerar el diagnóstico de bola fúngica sinusal en pacientes inmunocomprometidos en la práctica clínica y mantenerse alerta ante la posibilidad de infecciones fúngicas como efecto secundario del uso prolongado de corticosteroides.
Palabras clave: efectos colaterales; errores de medicación; hidrocortisona; infección fúngica; reacciones adversas relacionados con medicamentos.
Received: 23/04/2025
Approved: 04/08/2025
INTRODUCTION
Fungal rhinosinusitis is a medical condition categorized into invasive and noninvasive types based on histopathological examination.(1) The first, the invasive form, consists of spreading the fungus to adjacent tissues and is classified as acute fulminant, chronic, or chronic granulomatous disease.(2) On the other hand, the noninvasive form, such as a sinus fungal ball or allergic sinusitis, does not affect other structures.(3)
The prevalence of sinus fungal ball (SFB) is approximately 1 to 3 cases per 1,000 patients with chronic rhinosinusitis.(4) This condition, characterized by the accumulation of fungal elements within the paranasal sinuses, is considered an atypical form of chronic rhinosinusitis(4). Although the exact etiology of SFB formation is not yet fully understood, long-term use of corticosteroids has been identified as a potential risk factor.(5) Nevertheless, the limited number of reports describing this fungal infection as an adverse drug event may influence clinical decision-making.
A study revealed that patients with chronic fungal sinusitis are initially mistreated.(6,7) In patients with SFB, systemic or topical treatments are not appropriate because this infection is not invasive. This disease should be managed by functional endoscopic sinus surgery.(8) The quality of life of patients with SFB who receive delayed or inadequate treatment can be severely affected.
This document describes a case of SFB following long-term hydrocortisone use in a patient with autoimmune disease.
CLINICAL CASE
A 57-year-old male patient presented with left paranasal pain associated with productive cough with yellow-greenish expectoration in January 2023. He reported a history of Addison’s disease (AD) under treatment with oral hydrocortisone 30mg/12 hours 36 years ago. Based on the above data, a diagnosis of bacterial sinusitis was established, and antibiotic treatment was administered (amoxicillin and clavulanic acid 500/125mg every 12 hours for 7 days) together with an increase of hydrocortisone to 60-90mg every 12 hours.
After the initial treatment, levofloxacin 500 mg orally once daily for 10 days was prescribed. However, due to the absence of symptomatic relief, amoxicillin/clavulanic acid (500/125 mg administered orally (PO,) every 12 hours) was subsequently administered in combination with acetylcysteine (200 mg PO every 8 hours) for 7 days, resulting in clinical improvement.
Nonetheless, 7 months (July) after the first visit, the patient was hospitalized for decompensation, so hydrocortisone 30mg every 4-6 hours (PO), associated with ceftriaxone IV 2g every 24 hours for 3 days, was administered.
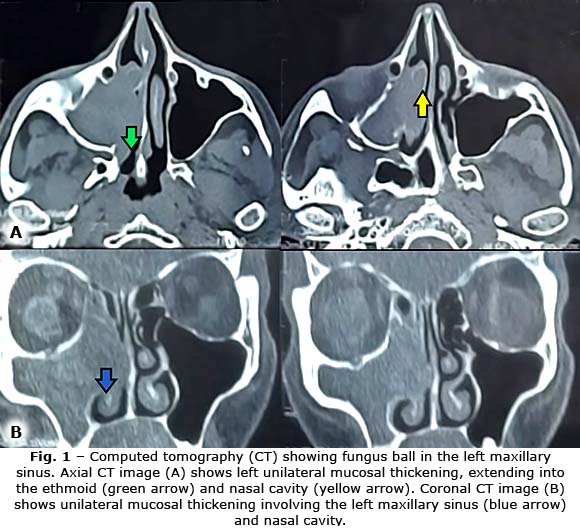
After hospitalization, a computed tomography (CT) scan was performed. Pseudopneumatization of the left maxillary sinus with an oval shape (31 mm × 15 mm) was observed, which was compatible with a fungal ball. This breached the medial wall of the left maxillary sinus, extending toward the nasal cavity and the ethmoidal cavity, and thickening the left maxillary mucosa (Fig. 1).
Subsequently, the medical personnel attempted to perform a nasal secretion culture, but the results were negative. Then, the physician decided not to prescribe more drugs to the patient, as this fungal ball was located in a poorly irrigated cavity and systemic drugs could not have an effect. The surgery to remove this fungal ball was scheduled for September (two months after the results of the CT scan). Unfortunately, during this waiting period, the patient continued to experience sinus pain, cough with sputum, and complications related to AD. In addition, the patient suffered two decompensations related to electrolyte disturbances, and he had to be hospitalized.
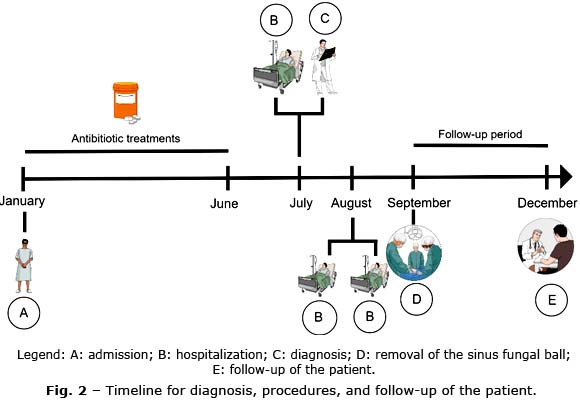
Finally, after surgery, he received antibiotic therapy with ciprofloxacin 500mg every 12 hours for 7 days, loratadine 10mg every 24 hours for 10 days, and analgesic treatment with naproxen 500 mg and paracetamol 500 mg for 5 days. The patient was followed up for 3 months and presented a favorable course without complications (Fig. 2), and also gave informed consent for the publication of the case.
The adapted Naranjo algorithm,(9) was used to establish causality between hydrocortisone and SFB, as well as the Hartwig Severity Assessment Scale.(10;11) to assess the severity of the adverse drug event. A "possible" level of causality was found with a level 4 (moderate) severity.
COMMENTS
Despite the increasing prevalence of SFB,(12) this disease is still treated as a rare condition in medical practice.(13) In addition, the diagnosis of fungal rhinosinusitis is particularly difficult because the clinical presentation is not specific and can occasionally be misleading. Consequently, misdiagnosis and mistreatment may be common in patients with fungal infections.
In this case report, the patient received antibiotics for suspected bacterial sinusitis in the first six months. The use of antibiotics could complicate the patient’s medical condition since he had a history of an autoimmune disorder and long-term treatment with corticosteroids. Furthermore, the risk of tendinopathy or tendon rupture associated with fluoroquinolones, such as levofloxacin, can increase in patients who use concomitant systemic corticoids.(14)
Another relevant point in this case was the delay in diagnosis and treatment, with the patient requiring three hospitalizations before receiving appropriate care. In Peru, healthcare delays remain a critical problem. A study found that 71.3% of the total population of Peru's Social Health Insurance who required medical attention received appropriate medical care after three months.(15)
Causality between hydrocortisone and SFB was possible in this case. This drug suppresses the immune system and can increase the risk of fungal infection in susceptible individuals.(6) However, SFB is a multifactorial disease. In the patient, not only immunosuppression but also the autoimmune disorder(16) of the patient could have contributed to the development of this fungal infection.
The potential side effects of fungal infection with hydrocortisone are rarely reported. This disease accounted for 4% of the total ADRs reported in VigiAccess. However, the database does not specify whether any cases of SFB were reported within this category.(17) This lack of information can also lead to misdiagnosis and mistreatment of SFB patients. It is important to determine the association between this drug use and the development of this particular condition. Therefore, further investigation and surveillance are needed to gain a clearer understanding of the potential risks of hydrocortisone therapy to SFB occurrence.
Healthcare professionals should remain vigilant and alert to the possibility of fungal infections as a potential side effect of long-term corticosteroid treatment.
Ethics and Consent
The patient provided informed consent, authorizing the publication of general information while ensuring the exclusion of any personal identifiers.
BIBLIOGRAPHIC REFERENCES
1. Akhondi H, Woldemariam B, Rajasurya V. Fungal Sinusitis. (In: StatPearls, ed.). Treasure Island (FL) [Internet]. StatPearls Publishing. 2024. [acceso: 13/10/2024]. Disponible en: https://pubmed.ncbi.nlm.nih.gov/31855340/
2. Alarifi I, Alsaleh S, Alqaryan S, et al. Chronic Granulomatous Invasive Fungal Sinusitis: A Case Series and Literature Review [Internet]. Ear, Nose Throat J. 2021; 100(5_suppl):720S-727S. DOI: 10.1177/0145561320904620
3. Marple BF, Gibbs SR, Newcomer MT, Mabry RL. Allergic fungal sinusitis-induced visual loss [Internet]. Am J Rhinol. 1999; 13(3):191-5. DOI: 10.2500/105065899781389740
4. Nassrallah S, Neagoş CM, Mocan SL, Neagoş A. Evaluation of the incidence of inflammatory and tumor pathology of nose and nasal sinus region [Internet]. Rom J Morphol Embryol. 2020; 61(4):1295-300. DOI: 10.47162/RJME.61.4.30
5. Ghogomu N, Kern R. Chronic rhinosinusitis: the rationale for current treatments [Internet]. Expert Rev Clin Immunol. 2017; 13(3):259-70. DOI: 10.1080/1744666X.2016.1220833
6. Wallis RS, Broder MS, Wong JY, Hanson ME, Beenhouwer DO. Granulomatous Infectious Diseases Associated with Tumor Necrosis Factor Antagonists [Internet]. Clin Infect Dis. 2004; 38(9):1261-5. DOI: 10.1086/383317
7. Ponikau JU, Sherris DA, Kern EB, Homburger HA, Frigasc E, Gaffey TA, et al. The Diagnosis and Incidence of Allergic Fungal Sinusitis [Internet]. Mayo Clin Proc. 1999; 74(9):877-84. DOI: 10.4065/74.9.877
8. Deutsch PG, Whittaker J, Prasad S. Invasive and Non-Invasive Fungal Rhinosinusitis-A Review and Update of the Evidence [Internet]. Medicina (Kaunas). 2019; 55(7):55070319. DOI: 10.3390/medicina55070319
9. Kelly WN, Arellano FM, Barnes J. Guidelines for submitting adverse event reports for publication [Internet]. Pharmacoepidemiol Drug Saf. 2007; 16(5):581-7. DOI: 10.1002/pds.1399
10. Naranjo CA, Busto U, Seller EM . Naranjo Adverse Drug Reaction Probability Scale. Clin Pharmacol Ther [Internet]. 1981; 30(2):239-45. DOI: 10.1038/clpt.1981.154
11. Hartwig SC, Siegel J, Schneider PJ. Preventability and severity assessment in reporting adverse drug reactions [Internet]. Am J Hosp Pharm. 1992 [acceso: 31/11/2024]; 49(9):2229-32. Disponible en: https://pubmed.ncbi.nlm.nih.gov/1524068/
12. Lee JS, Shin SY, Lee KH, Kim SW, Cho JS. Change of prevalence and clinical aspects of fungal ball according to temporal difference [Internet]. Eur Arch Oto-Rhino-Laryngology. 2013; 270(5):1673-7. DOI: 10.1007/s00405-012-2234-x
13. Yağmur AR, Çufalı ÖF, Çolak M, Çufal A, Kayal SA, Yeniçeri A, et al. Invasive fungal rhinosinusitis, clinical manifestations, and prognostic values: as case series audit [Internet]. Egypt J Otolaryngol. 2023; 39(1). DOI: 10.1186/s43163-023-00551-8
14. Wise BL, Peloquin C, Choi H, Lane NE, Zhang Y. Impact of age, sex, obesity, and steroid use on quinolone-associated tendon disorders [Internet]. Am J Med. 2012; 125(12):1228.e23-1228.e28. DOI: 10.1016/j.amjmed.2012.05.027
15. Llanos RQ, Ramírez RR, Palacios MT, Flores CF, Borda-Olivas A, Castillo RA, et al. Health Survey in a Peruvian health system (ENSSA): design, methodology and general results [Internet]. Rev Saude Publica. 2019; 53:33. DOI: 10.11606/S1518-8787.2019053001135
16. Bhattacharya S, Kubiha S, Tyagi P. Fungi and Endocrine Dysfunction. In: Feingold KR, Anawalt B, Blackman MR. Editorial: South Dartmouth (MA): MDText.com, Inc.; [Internet]. 2000. [acceso: 20/10/2024]. Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK572246/
17. World Health Organization. Global Programme on Evidence for Health Policy. [Internet]. VigiAccess; 2024. [acceso: 22/10/2024]. Disponible en: https://www.vigiaccess.org/
Conflicts of Interest
The authors have no conflicts of interest to declare.
Financial Information
Not applied.
Data Availability
The data used for this case report correspond to the Regional Hospital of Ica, Peru.