Systematic Review
Risk of breast cancer in people with periodontal disease: a systematic review and meta-analysis
Riesgo de cáncer de mama en personas con enfermedad periodontal: una revisión sistemática y metaanálisis
Fiki Muhammad Ridho1
https://orcid.org/0000-0002-0187-8160
Siska Maulidina Cahyani2
https://orcid.org/0009-0008-8340-8672
Ridwan Alfatah3
https://orcid.org/0009-0004-1940-5216
Alfi Syahri4,5,6
https://orcid.org/0009-0009-8756-6288
Anis Irmawati7*
https://orcid.org/0000-0002-6568-6512
1Universitas Airlangga. Faculty of Dental Medicine. Department
of Dental Medicine. Surabaya, Indonesia.
2Universitas Brawijaya. Faculty of Dentistry. Malang, Indonesia.
3Universitas Islam Negeri Walisongo. Faculty of Medicine.
Semarang, Indonesia.
4Universitas Airlangga. Faculty of Nursing. Department of
Surgical Medical Nursing. Surabaya, Indonesia.
5Universitas Airlangga. Faculty of Nursing. Surabaya, Indonesia.
6Institut Kesehatan Deli Husada. Faculty of Nursing. Department
of Advanced Nursing. Deli Serdang, Indonesia.
7Universitas Airlangga. Faculty of Dental Medicine. Department
of Oral Biology. Surabaya, Indonesia.
*Corresponding author. Email: anis-m@fkg.unair.ac.id
ABSTRACT
Introduction: Periodontal disease (PD) has been associated with the
incidence of chronic systemic diseases, including breast cancer (BC).
However, studies on their association have shown inconsistent results.
Objective: To evaluate the risk of BC in people with PD.
Methods: A systematic review and meta-analysis following the PRISMA
2020 guidelines in Scopus, PubMed, ScienceDirect, EBSCO, Wiley Online
Library, and Google Scholar was performed. Any observational study
evaluating BC risk in people with and without PD was included. Study
quality assessment was conducted using the Newcastle-Ottawa Scale. Fixed-
or random-effects model meta-analyses were used and the results were
reported as relative risks (RR) and 95% confidence intervals (CI). All
statistical analyses were performed using Stata version 17.0 software.
Results: Fifteen observational studies involving 816,219 female
participants were included. There was a 22% increased risk of BC in people
with PD (RR = 1.22; 95% CI = 1.10-1.35; p = 0.0001; I2
= 89.80%). Subgroup analysis showed consistent and significant results when
stratified by sample size and follow-up period. This meta-analysis was
robust based on sensitivity analysis; however, it should be interpreted
with caution due to its high heterogeneity.
Conclusions: The risk of BC is increased in people with PD. Future
studies are needed to evaluate the effect of periodontal treatment on
reducing the risk of BC.
Keywords: breast cancer; meta-analysis; oral health; periodontal disease; periodontitis.
RESUMEN
Introducción: La enfermedad periodontal (PD) se ha asociado con la
incidencia de enfermedades sistémicas crónicas, incluido el cáncer de mama
(BC). Sin embargo, los estudios sobre su asociación han mostrado resultados
inconsistentes.
Objetivo: Evaluar el riesgo de BC en personas con PD.
Métodos: Se realizó una revisión sistemática y metaanálisis
siguiendo las pautas PRISMA 2020 en Scopus, PubMed, ScienceDirect, EBSCO,
Wiley Online Library y Google Scholar. Se incluyó cualquier estudio
observacional que evaluara el riesgo de BC en personas con y sin PD. La
evaluación de la calidad del estudio se realizó utilizando la escala
Newcastle-Ottawa. Se utilizaron metaanálisis de modelos de efectos fijos o
aleatorios y los resultados se informaron como riesgos relativos (RR) e
intervalos de confianza del 95 % (CI). Todos los análisis estadísticos se
realizaron utilizando el software Stata versión 17.0.
Resultados: Se incluyeron quince estudios observacionales que
involucraron a 816.219 participantes femeninas. Se observó un aumento del
22 % en el riesgo de BC en personas con PD (RR= 1,22; 95 % CI= 1,10-1,35; p= 0,0001; I2= 89,80 %). El análisis de subgrupos
mostró resultados consistentes y significativos cuando se estratificó por
tamaño de muestra y período de seguimiento. Este metaanálisis fue sólido
según el análisis de sensibilidad; sin embargo, debe interpretarse con
cautela debido a su alta heterogeneidad.
Conclusiones: El riesgo de BC aumenta en personas con PD. Se
necesitan futuros estudios para evaluar el efecto del tratamiento
periodontal en la reducción del riesgo de BC.
Palabras clave: cáncer de mama; enfermedad periodontal; metaanálisis; periodontitis; salud bucal.
Received: 20/05/2025
Approved: 19/06/2025
INTRODUCTION
Periodontal disease (PD) is a chronic inflammatory disease of the tooth supporting tissue or periodontium, causing tissue damage and contributing to systemic chronic inflammation.(1) Accumulation of periodontal pathogenic bacteria and biofilm on teeth is considered to be the main factor in the occurrence of PD.(2) Currently, PD remains recognized as a global public health issue that needs to be addressed, with 1.1 billion cases and 91 million new cases of PD identified in 2019.(3) In addition to having a negative impact on oral health, PD also contributes to an increased risk of various chronic systemic conditions, including diabetes,(4) cardiovascular disease,(5) metabolic syndrome,(6) rheumatoid arthritis,(7) adverse pregnancy outcomes,(8,9) respiratory diseases,(10) chronic kidney disease,(11) cognitive impairment,(12) male reproductive health problems,(13,14) and various types of intraoral and extraoral cancer.(15)
Breast cancer (BC) is one of the most common types of deadly cancer in women, becoming a complex global health problem. Based on global epidemiological data in 185 countries obtained from GLOBOCAN, as many as 2.1 million cases and more than 600 thousand deaths due to BC were identified in 2018,(16) and increased to 2.26 million cases in 2020, making BC the most frequently diagnosed cancer globally among other cancers.(17) Various risk factors for BC include female gender, age, family history, BRCA gene mutations, pregnancy, menstrual periods and menopause.(18) In addition, alcohol consumption, smoking, lifestyle, diet, consumption of certain medications, and obesity are modifiable risk factors that contribute to the occurrence of BC.(19)
Mechanistic evidence between PD and the risk of various cancers has been observed, including the development of BC.(20) Oral pathogens are considered to be factors that have strong potential to enter the bloodstream and spread to other organs.(21) Periodontal pathogens have been shown to induce carcinogenesis through the interaction of integrin and Toll-like receptor 4 (TLR4)/MyD88 signaling pathways, further contributing to BC cell metastasis.(22) In addition, chronic inflammation caused by PD triggers systemic inflammation. Inflammatory mediators produced by periodontal pathogens are suggested to be associated with oncogene activation, cell cycle inhibition, cell proliferation, mutagenesis, DNA damage, angiogenesis, and metastasis.(23)
Studies investigating the relationship between PD and the risk of BC incidence have been conducted. However, their results have shown inconsistent results, with some studies showing a significant association;(24,25,26) however, other studies revealing no increased risk of BC in people with PD.(27,28,29) Therefore, this study aims to identify the pooled risk of BC in people with PD using meta-analysis.
METHODS
Protocol and focused question
This study is a systematic review and meta-analysis followed the PRISMA 2020 guidelines.(30) The research question of this study was "What is the risk of BC in people with PD?". The population, exposure, comparison, outcome, and study (PECOS) framework was used to address the research questions, with P: any population; E: PD; C: population without PD or healthy controls; O: risk of BC; and S: cohort, case-control, or cross-sectional studies.
Search strategy
A systematic and comprehensive literature search in Scopus, PubMed, ScienceDirect, EBSCO, Wiley Online Library, and Google Scholar from inception to December 2024 was performed. The following are the terms used in literature searches: periodontal OR periodontal disease OR periodontitis OR oral health AND breast OR breast cancer OR breast neoplasm OR cancer.
Eligibility criteria
Articles were included if they: 1) were cohort, case-control, or cross-sectional studies, 2) observed the risk of BC in people with PD, 3) used study subjects from a population diagnosed with PD and control subjects from a population without PD, 4) reported risk relative (RR), odds ratio (OR), or hazard ratio (HR) along with 95% confidence interval (CI), and 5) were full-text and peer-reviewed. In contrast, all review articles, commentaries, letters to editors, short communications, case reports, and case series were excluded from this study. Authors strictly addressed studies that have the potential for data or sample duplication using the same dataset, if any, where studies that involve more samples or use a longer time span and/or studies that use more rigorous and comprehensive research methods were selected. This was a concern to reduce selection bias and increase the validity of meta-analysis results. Finally, other restraints were not applied in the study selection, including publication year and language restrictions. Therefore, all observational articles published until December 2024 were considered for inclusion.
Quality assessment
Newcastle-Ottawa Scale (NOS) was employed for the quality assessment of included studies.(31) The NOS has three components: selection, comparability, and results, with overall score ranges from 0 to 9. Study quality was assessed as high if the overall score was ≥7, moderate if the overall score was 4-6, and poor if the overall score was ≤3. Study quality was assessed by two reviewers (F.M.R. and A.S.) and validated by a senior researcher (A.I.). Any discrepancies during the assessment of study quality were addressed through in-depth discussion between authors and careful decision making.
Data extraction
Independently, two authors (F.M.R. and A.S.) performed data extraction from included studies using table containing reference, country, study design, sample size, age, PD assessment, BC assessment, adjustments for confounding factors, and estimates (RR, OR, or HR) with 95% CI. All data were processed quantitatively and qualitatively to draw definite conclusions.
Statistical analysis
Risk of BC in people with PD was measured using meta-analysis and presented as adjusted RR and 95% CI, with a p-value considered statistically significant being <0.05. Estimates in the form of OR or HR were considered as RR when performing a pooled analysis. Heterogeneity test (I2) was performed to evaluate data variation between included studies, where low heterogeneity was stated if I2 was ≤50% or p ≥0.1 and high heterogeneity if I2 was >50% or p <0.1. Referring to the results of the heterogeneity test, a fixed-effects model meta-analysis was selected if the heterogeneity was low, whereas a random-effects model was used otherwise. Subgroup analysis was also performed to evaluate the significance and consistency of the meta-analysis results stratified by country, study design, sample size, follow-up period, periodontal assessment, and BC assessment. Sensitivity analysis was conducted to evaluate the robustness of the meta-analysis results, using the leave-one-out method by omitting one study at a time and recalculating the pooled RR and its 95% CI.(32)
Initially, a funnel plot was used to identify possible publication bias, in accordance with the consensus that a funnel plot can be used if the number of included studies is more than 10 studies.(33) In addition, publication bias was also assessed using the Egger regression test(34) and the Begg and Mazumdar nonparametric rank correlation test,(35) with a p-value of >0.05 considered no publication bias was observed. All statistical analyses were performed using Stata version 17.0 software.
RESULTS
Study selection
After removing duplicate articles, 1,137 potential articles were identified from the electronic database search. Initial screening of the records was then performed and 904 articles were excluded, leaving 233 papers. In the next selection stage, 197 articles were not retrieved based on the irrelevance of the title and abstract. The remaining 36 articles were subjected to a thorough eligibility assessment, excluding 22 reports for the following reasons: article not available (n = 2), unspecified data (n = 5), reviews articles (n = 6), issues in study methods (n = 4), ineligible comparison (n = 3), and articles using the same dataset (n = 2). A manual search through other sources was also conducted to minimize study selection bias, finding two studies, but one study had to be excluded because the article was not available. Finally, fifteen studies were included in this meta-analysis (Fig. 1 - See with original resolution).
Characteristics of included studies
This study included 15 observational studies involving 816,219 female participants aged 19 years or older. The included studies consisted of nine prospective cohort,(25,27,29,36,37,38,39,40,41) three retrospective cohort,(26,28,42) and three case-control studies.(24,43,44)
Studies using a cohort design, the follow-up period varied from 2 to 27 years. The participants involved came from the following regions: Asia including Taiwan(24,26,42) and South Korea;(38) Europe including Sweden,(36,41) Greece,(43) and Finland;(28) North America including the USA;(25,27,29,37,39,40) and South America including Brazil.(44)
In assessing PD, several methods/criteria were used: self-report,(27,29,36,37) ICD,(24,26,39,42) oral examination,(41,43) CPI score,(38) medical records,(28) radiographic alveolar crestal bone height,(40) and CDC-AAP criteria.(25,44) Meanwhile, assessment for BC was carried out using the following methods/criteria: ICD,(24,26,28,29,36,37,39,41,42,44) medical records,(25,40,43) and self-report.(27,38) A table of characteristics of included studies is available in the supplementary file.
Quality assessment of included studies
Based on the results of the quality assessment of the included studies, six studies(26,27,28,29,42,44) obtained an overall score of 9, five studies(24,25,37,38,40) obtained an overall score of 8, and four studies(36,39,41,43) were assessed with an overall score of 7. Overall, the studies included were of high quality.
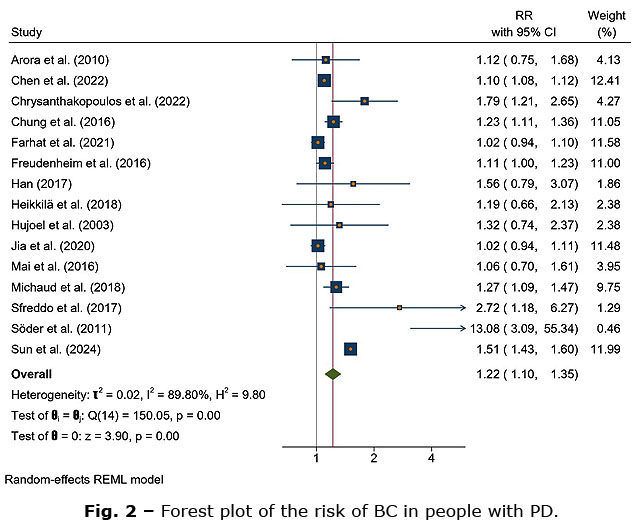
Risk of breast cancer inpeople with periodontal disease
The results of the random-effects model meta-analysis showed a statistically significant increase in the risk of BC of 22% in people with PD (RR = 1.22; 95% CI = 1.10-1.35; p = 0.0001). Interpretation of this meta-analysis should be done with caution because the heterogeneity test showed that the studies were heterogeneous (I2 = 89.80%; p = 0.00) (Fig. 2).
Subgroup analysis of the risk of breast cancer in people with periodontal disease
Given the diversity of characteristics of the included studies, authors subsequently performed subgroup analyses stratified by country, study design, sample size, follow-up period, PD assessment, and BC assessment, described in table 1.
Subgroup meta-analysis stratified by country found significant and consistent results in Asian (RR = 1.28; p = 0.005), North American (RR = 1.06; p = 0.01), and South American populations (RR = 2.72; p = 0.02), but not in European populations (RR = 1.93; p = 0.12).
Based on study design, the risk of BC in people with PD was consistent across prospective cohort (RR = 1.10; p = 0.02) and retrospective cohort study designs (RR = 1.36; p = 0.0008), but not across case-control studies (RR = 1.56; p = 0.08).
BC risk in the PD people also consistently increased based on sample size, both in studies with samples <10,000 (RR = 1.41; p = 0.0005) and ≥10,000 (RR = 1.16; p = 0.02), and based on follow-up period, both in studies with follow-up periods <10 years (RR = 1.12; p = 0.03) and ≥10 years (RR = 1.25; p = 0.006). When stratified by PD assessment, significant and consistent results were observed in studies with ICD (RR = 1.27; p = 0.005) and medical records (RR = 1.19; p = 0.006), while inconsistent results were found in self-report (RR = 1.04; p = 0.12), oral/radiographic examination (RR = 2.49; p = 0.18), CDC-AAP (RR = 1.66; p = 0.16), and CPI score (RR= 1.56; p = 0.20).
Meanwhile, based on the criteria for BC diagnosis, studies using ICD as BC assessment showed consistent results (RR = 1.27; p = 0.0004), but were not significant in studies using medical records (RR = 1.21; p = 0.08) and self-report (RR = 1.03; p = 0.52).
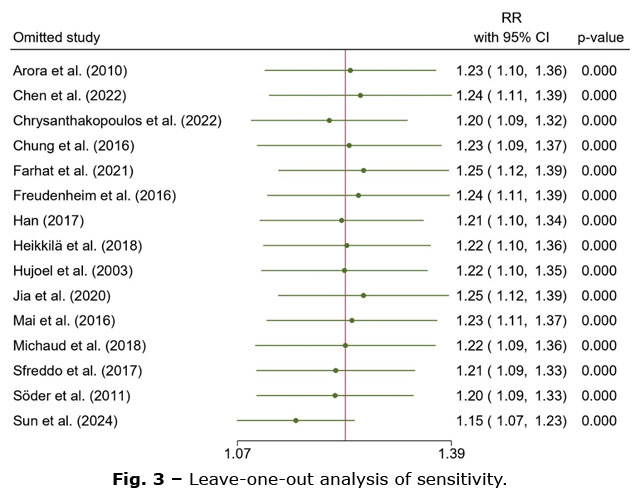
Sensitivity analysis
To determine the robustness of the results, sensitivity analysis was subsequently conducted by removing studies one by one and recalculating the remaining studies. The results showed stable pooled RR, 95% CI, and p -value, no significant changes were observed, concluding that this meta-analysis is robust (Fig. 3).
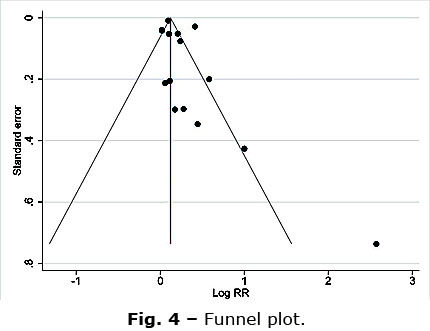
Publication bias
The results of the funnel plot revealed an asymmetric distribution of studies (Fig. 4). To confirm the funnel plot results, authors also conducted the Egger regression test ( p = 0.0055) and the Begg and Mazumdar nonparametric rank correlation test ( p = 0.0478). Based on these results, publication bias was observed.
DISCUSSION
The results of this study revealed a significant increase in the risk of BC in people with PD by 22%. The subgroup analyses of this meta-analysis were also consistent when stratified by sample size and follow-up period, but inconsistent when stratified by country, study design, periodontal assessment, and BC assessment.
Nonetheless, this meta-analysis should be interpreted with caution, given that heterogeneity tests showed substantial variation between studies. These differences are believed to be caused by factors such as population characteristics, sample size, study design, and/or measurement methods used in each study. In addition, the high heterogeneity among studies is likely due to differences in the confounding factors adjusted for. The results of the publication bias analysis indicated publication bias, which may affect the interpretation of the results. However, sensitivity analysis showed that the meta-analysis results remained stable, indicating that the effect estimates were not dependent on a single study. In conclusion, this meta-analysis should be interpreted with caution despite their robustness.
Previous meta-analyses by Sha o J et al.(45) and Shi T et al.(46) both conducted in 2018 and involving approximately 180 thousand samples showed significant results. However, one of these meta-analyses included studies that were excluded in this meta-analysis on the grounds of ineligible comparison, where one study(47) did not use a control/comparison group in its research subjects. Furthermore, the two previous meta-analyses need to be updated to incorporate newer studies with larger study samples. Therefore, this meta-analysis is currently the latest and most comprehensive, involving larger study samples from additional studies.
Mechanisms of PD in increasing BC risk have been proposed. Strong suspicion arises from chronic periodontal inflammation that has systemic effects. Oral microbiota promote genomic instability, chronic inflammation, mutation accumulation, and cancer development through specific substances produced by them.(23) Furthermore, people with PD have increased levels of C-reactive protein (CRP) and the transcription factors, receptor activator of nuclear factor kappa B (RANK) and RANK ligand (RANKL).(22,48 ) Higher risk of systemic diseases has been linked to systemically raised CRP levels, including higher risk of BC.(49 ) Meanwhile, increased transcription factors RANK and RANKL are believed to induce the formation of pre-neoplastic and invasive tumors in the breast.(50)
Periodontal pathogens, such as Porphyromonas gingivalis and Fusobacterium nucleatum, were reported to produce lipopolysaccharides (LPS) that contribute to chronic inflammation and potentially increase the risk of BC.(51) LPS from oral pathogens has been documented to increase inflammatory protein expression, nuclear factor kappa β (NF-κβ) activation, and anti-apoptotic BCL-2 and BCL-xL expression.(52) This may occur via immune receptors such as TLR4, which in turn serves to increase more inflammatory and cancer-related chemokines and cytokines.(53) In addition, F. nucleatum increases matrix metalloproteinase-9 (MMP-9), triggers inflammatory responses and facilitates a microenvironment that promotes carcinogenesis.(54) Furthermore, P. gingivalis have carcinogenic properties such as preventing cell apoptosis, growing and surviving in epithelial cells and spreading to other organs, inducing cellular proliferation, activating cyclooxygenase-2 (COX-2) gene expression, and increasing the production of tumor necrosis factor-α (TNF-α), interleukin (IL)-6, IL-8, and IL-1β.(55) In conclusion, systemic chronic inflammation and activation of various inflammatory biomarkers by periodontal pathogens and their toxins contribute to carcinogenesis, leading to increased risk of BC.
The findings of this meta-analysis suggest an increased risk of BC in individuals with PD, which provides a clinically important signal regarding a possible association between periodontal health and BC risk. However, the high heterogeneity among the studies analyzed suggests that these results should be interpreted with caution. Therefore, although the potential for PD as a risk factor for BC is noteworthy, the current evidence is insufficient to provide a basis for changes in policy or clinical guidelines. Nevertheless, it is important for healthcare professionals to begin to raise clinical awareness of this possible association. Given that PD is a chronic disease that can be modified through preventive and therapeutic interventions, evaluation of periodontal status can be considered as part of a comprehensive screening and holistic approach in early detection of BC risk, especially in women with additional risk factors.
The findings also provide a rational basis for collaboration between dentists and medical personnel in integrating aspects of oral health and systemic health. In the future, more rigorous longitudinal studies and intervention trials are needed to establish a causal relationship between these two conditions and to assess whether periodontal management can contribute to BC prevention efforts.
This study has several strengths. First, this meta-analysis is the most recent and comprehensive to date, with updated studies and involving a larger sample. Second, the literature search was conducted systematically and comprehensively from various electronic databases and manual searches with strict eligibility assessment, reducing study selection bias. Third, the quality assessment of the included studies showed high study quality. Fourth, the pooled estimation results have been adjusted for confounding factors; therefore, the results are not influenced by other factors. Fifth, the sensitivity analysis showed that the results of this meta-analysis were robust.
However, this meta-analysis also acknowledges several limitations. First, the included studies had high variation as indicated by high heterogeneity test results, making this meta-analysis must be interpreted with caution. Second, publication bias exists, indicated by the results of visual interpretation with funnel plot and confirmed by Egger's test and Begg and Mazumdar's test. Third, there is a controversy in establishing the diagnosis of PD, where several studies used appropriate clinical criteria such as CDC-AAP, ICD, oral and radiographic examination, and CPI score, but several others used self-report methods. This is certainly a concern because it is prone to bias, where it is possible for periodontally healthy people to be included in the PD group, and vice versa. Therefore, the use of the latest criteria for establishing the diagnosis of PD is highly recommended for future research.(56)
In conclusion, this meta-analysis revealed a significantly increased risk of BC in people with PD. This is believed to be due to the periodontal inflammatory response and toxins from periodontal pathogens that cause systemic chronic inflammation and initiate BC-causing factors. This meta-analysis involved observational studies that could not evaluate causal relationships, so this study requires future studies with rigorous methods to analyze the causal relationship between PD and increased risk of BC. In addition, studies related to the provision of periodontal treatment interventions to reduce the risk of BC need to be conducted, considering that studies related to this are rarely conducted.
BIBLIOGRAPHIC REFERENCES
1. Kinane DF, Stathopoulou PG, Papapanou PN. Periodontal diseases [Internet]. Nat Rev Dis Primers. 2017;3(1):17038. DOI: 10.1038/nrdp.2017.38
2. Sedghi LM, Bacino M, Kapila YL. Periodontal Disease: The Good, The Bad, and The Unknown [Internet]. Front Cell Infect Microbiol. 2021;11:766944. DOI: 10.3389/fcimb.2021.766944
3. Zhang X, Wang X, Wu J, Wang M, Hu B, Qu H, et al. The global burden of periodontal diseases in 204 countries and territories from 1990 to 2019 [Internet]. Oral Diseases. 2024;30(2):754-68. DOI: 10.1111/odi.14436
4. Stöhr J, Barbaresko J, Neuenschwander M, Schlesinger S. Bidirectional association between periodontal disease and diabetes mellitus: a systematic review and meta-analysis of cohort studies [Internet]. Sci Rep. 2021 Jul 1;11(1):13686. DOI: 10.1038/s41598-021-93062-6
5. Larvin H, Kang J, Aggarwal VR, Pavitt S, Wu J. Risk of incident cardiovascular disease in people with periodontal disease: A systematic review and meta‐analysis [Internet]. Clinical & Exp Dental Res. 2021;7(1):109-22. DOI: 10.1002/cre2.336
6. Gobin R, Tian D, Liu Q, Wang J. Periodontal Diseases and the Risk of Metabolic Syndrome: An Updated Systematic Review and Meta-Analysis [Internet]. Front Endocrinol. 2020 Jun 9;11:336. DOI: 10.3389/fendo.2020.00336
7. Qiao Y, Wang Z, Li Y, Han Y, Zhou Y, Cao X. Rheumatoid arthritis risk in periodontitis patients: A systematic review and meta-analysis [Internet]. Joint Bone Spine. 2020;87(6):556-64. DOI: 10.1016/j.jbspin.2020.04.024
8. Chen P, Hong F, Yu X. Prevalence of periodontal disease in pregnancy: A systematic review and meta-analysis [Internet]. Journal of Dentistry. 2022;125:104253. DOI: 10.1016/j.jdent.2022.104253
9. Ridho FM, Algifnita AO, Pramaztri NN, Laksono EP, Allifiah BPN, Ahmad M. Periodontitis as a Risk Factor of Preeclampsia in Pregnancy: A Scoping Review [Internet]. International Islamic Medical Journal. 2024;5(2):9-25. DOI: 10.33086/iimj.v5i2.5316
10. Gomes‐Filho IS, Cruz SSD, Trindade SC, Passos‐Soares JDS, Carvalho‐Filho PC, Figueiredo ACMG, et al. Periodontitis and respiratory diseases: A systematic review with meta‐analysis [Internet]. Oral Diseases. 2020;26(2):439-46. DOI: 10.1111/odi.13228
11. Deschamps‐Lenhardt S, Martin‐Cabezas R, Hannedouche T, Huck O. Association between periodontitis and chronic kidney disease: Systematic review and meta‐analysis [Internet]. Oral Diseases. 2019 Mar;25(2):385-402. DOI: 10.1111/odi.12834
12. Guo H, Chang S, Pi X, Hua F, Jiang H, Liu C, et al. The Effect of Periodontitis on Dementia and Cognitive Impairment: A Meta-Analysis [Internet]. IJERPH. 2021;18(13):6823. DOI: 10.3390/ijerph18136823
13. Ridho FM, Agustina AW, Hidayati NN, Pratama MI, Laksono EP. Exploring the Association between Periodontitis and Erectile Dysfunction: A Systematic Review [Internet]. Indonesian Andrology and Biomedical Journal. 2024;5(1):42-51. DOI: 10.20473/iabj.v5i1.56744
14. Ridho FM, Alfatah R, Cahyani SM, Rahmawati RS. Association between periodontitis and sperm quality: a systematic review and meta-analysis [Internet]. Rwanda Medical Journal. 2025;82(2):55-66. DOI: 10.4314/rmj.v82i2.7
15. Corbella S, Veronesi P, Galimberti V, Weinstein R, Del Fabbro M, Francetti L. Is periodontitis a risk indicator for cancer? A meta-analysis [Internet]. PLoS ONE. 2018;13(4):e0195683. DOI: 10.1371/journal.pone.0195683
16. Sharma R. Global, regional, national burden of breast cancer in 185 countries: evidence from GLOBOCAN 2018 [Internet]. Breast Cancer Res Treat. 2021;187(2):557-67. DOI: 10.1007/s10549-020-06083-6
17. Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: An overview [Internet]. Intl Journal of Cancer. 2021;149(4):778-89. DOI: 10.1002/ijc.33588
18. Obeagu EI, Obeagu GU. Breast cancer: A review of risk factors and diagnosis [Internet]. Medicine. 2024;103(3):e36905. DOI: 10.1097/MD.0000000000036905
19. Łukasiewicz S, Czeczelewski M, Forma A, Baj J, Sitarz R, Stanisławek A. Breast Cancer-Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies-An Updated Review [Internet]. Cancers. 2021;13(17):4287. DOI: 10.3390/cancers13174287
20. Baima G, Minoli M, Michaud DS, Aimetti M, Sanz M, Loos BG, et al. Periodontitis and risk of cancer: Mechanistic evidence [Internet]. Periodontology 2000. 2024;96(1):83-94. DOI: 10.1111/prd.12540
21. Gaba FI, González RC, Martïnez RG. The Role of Oral Fusobacterium nucleatum in Female Breast Cancer: A Systematic Review and Meta-Analysis [Internet]. International Journal of Dentistry. 2022 Nov 23;2022:1-12. DOI: 10.1155/2022/1876275
22. Zhang Y, Ren X, Hu T, Cheng R, Bhowmick NA. The Relationship Between Periodontal Disease and Breast Cancer: From Basic Mechanism to Clinical Management and Prevention [Internet]. Oral Health Prev Dent. 2023;21:49-60. DOI: 10.3290/j.ohpd.b3904343
23. Issrani R, Reddy RJ, El-Metwally TH, Prabhu N. Periodontitis as a Risk Factor for Breast Cancer - What We Know Till Date? [Internet]. Asian Pac J Cancer Prev. 2021;22(10):3109-14. DOI: 10.31557/APJCP.2021.22.10.3109
24. Chen CC, Ho WL, Lin CH, Chen HH. Stratified analysis of the association between periodontitis and female breast cancer based on age, comorbidities and level of urbanization: A population-based nested case-control study [Internet]. PLoS ONE. 2022;17(7):e0271948. DOI: 10.1371/journal.pone.0271948
25. Michaud DS, Lu J, Peacock-Villada AY, Barber JR, Joshu CE, Prizment AE, et al. Periodontal Disease Assessed Using Clinical Dental Measurements and Cancer Risk in the ARIC Study [Internet]. JNCI: Journal of the National Cancer Institute. 2018;110(8):843-54. DOI: 10.1093/jnci/djx278
26. Sun LM, Tsai FJ, Lin CL, Wu YH. Women with breast cancer exhibit a higher risk for periodontitis: A nationwide cohort study [Internet]. Journal of Dental Sciences. 2024;S1991790224003891. DOI: 10.1016/j.jds.2024.11.016
27. Farhat Z, Cadeau C, Eliassen AH, Freudenheim JL. Periodontal Disease and Breast Cancer Risk: Results from the Nurses' Health Study [Internet]. Cancer Epidemiology, Biomarkers & Prevention. 2021;30(9):1757-60. DOI: 10.1158/1055-9965.EPI-21-0257
28. Heikkilä P, But A, Sorsa T, Haukka J. Periodontitis and cancer mortality: Register‐based cohort study of 68,273 adults in 10‐year follow‐up [Internet]. Intl Journal of Cancer. 2018;142(11):2244-53. DOI: 10.1002/ijc.31254
29. Jia M, Wu Z, Vogtmann E, O'Brien KM, Weinberg CR, Sandler DP, et al. The Association Between Periodontal Disease and Breast Cancer in a Prospective Cohort Study [Internet]. Cancer Prevention Research. 2020;13(12):1007-16. DOI: 10.1158/1940-6207.CAPR-20-0018
30. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews [Internet]. BMJ. 2021;372:n71. DOI: 10.1136/bmj.n71
31. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses [Internet]. Eur J Epidemiol. 2010;25(9):603-5. DOI: 10.1007/s10654-010-9491-z
32. Bown MJ, Sutton AJ. Quality Control in Systematic Reviews and Meta-analyses [Internet]. European Journal of Vascular and Endovascular Surgery. 2010;40(5):669-77. DOI: 10.1016/j.ejvs.2010.07.011
33. Sedgwick P, Marston L. How to read a funnel plot in a meta-analysis [Internet]. BMJ. 2015;351:h4718. DOI: 10.1136/bmj.h4718
34. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test [Internet]. BMJ. 1997;315(7109):629-34. DOI: 10.1136/bmj.315.7109.629
35. Begg CB, Mazumdar M. Operating Characteristics of a Rank Correlation Test for Publication Bias [Internet]. Biometrics. 1994;50(4):1088. DOI: 10.2307/2533446
36. Arora M, Weuve J, Fall K, Pedersen NL, Mucci LA. An Exploration of Shared Genetic Risk Factors Between Periodontal Disease and Cancers: A Prospective Co-Twin Study [Internet]. American Journal of Epidemiology. 2010;171(2):253-9. DOI: 10.1093/aje/kwp340
37. Freudenheim JL, Genco RJ, LaMonte MJ, Millen AE, Hovey KM, Mai X, et al. Periodontal Disease and Breast Cancer: Prospective Cohort Study of Postmenopausal Women [Internet]. Cancer Epidemiology, Biomarkers & Prevention. 2016;25(1):43-50. DOI: 10.1158/1055-9965.EPI-15-0750
38. Han M. Oral Health Status and Behavior among Cancer Survivors in Korea Using Nationwide Survey [Internet]. IJERPH. 2017;15(1):14. DOI: 10.3390/ijerph15010014
39. Hujoel PP, Drangsholt M, Spiekerman C, Weiss NS. An Exploration of the Periodontitis-Cancer Association [Internet]. Annals of Epidemiology. 2003;13(5):312-6. DOI: 10.1016/S1047-2797(02)00425-8
40. Mai X, LaMonte MJ, Hovey KM, Freudenheim JL, Andrews CA, Genco RJ, et al. Periodontal disease severity and cancer risk in postmenopausal women: the Buffalo OsteoPerio Study [Internet]. Cancer Causes Control. 2016;27(2):217-28. DOI: 10.1007/s10552-015-0699-9
41. Söder B, Yakob M, Meurman JH, Andersson LC, Klinge B, Söder PÖ. Periodontal disease may associate with breast cancer [Internet]. Breast Cancer Res Treat. 2011;127(2):497-502. DOI: 10.1007/s10549-010-1221-4
42. Chung SD, Tsai MC, Huang CC, Kao LT, Chen CH. A population-based study on the associations between chronic periodontitis and the risk of cancer [Internet]. Int J Clin Oncol. 2016;21(2):219-23. DOI: 10.1007/s10147-015-0884-6
43. Chrysanthakopoulos NA, Vryzaki E. Assessment of Periodontal Disease Indices in Breast Cancer Patients: A Case-Control Study [Internet]. Cases. 2022;1(2):6. DOI: 10.35702/cases.10006
44. Sfreddo CS, Maier J, De David SC, Susin C, Moreira CHC. Periodontitis and breast cancer: A case‐control study [Internet]. Comm Dent Oral Epid. 2017;45(6):545-51. DOI: 10.1111/cdoe.12318
45. Shao J, Wu L, Leng WD, Fang C, Zhu YJ, Jin YH, et al. Periodontal Disease and Breast Cancer: A Meta-Analysis of 1,73,162 Participants [Internet]. Front Oncol. 2018 Dec 12;8:601. DOI: 10.3389/fonc.2018.00601
46. Shi T, Min M, Sun C, Zhang Y, Liang M, Sun Y. Periodontal disease and susceptibility to breast cancer: A meta‐analysis of observational studies [Internet]. J Clinic Periodontology. 2018;45(9):1025-33. DOI: 10.1111/jcpe.12982
47. Dizdar O, Hayran M, Guven DC, Yılmaz TB, Taheri S, Akman AC, et al. Increased cancer risk in patients with periodontitis [Internet]. Current Medical Research and Opinion. 2017;33(12):2195-200. DOI: 10.1080/03007995.2017.1354829
48. Ridho FM, Syachputra AJ, Nur'aini AD, Ulfah K, Faqih M, Nurhuda A. Pre-clinical and clinical efficacy of curcumin as an anti-inflammatory agent for periodontitis. A systematic review [Internet]. Revista Científica Odontológica. 2024;12(4):e222. DOI: 10.21142/2523-2754-1204-2024-222
49. Guo L, Liu S, Zhang S, Chen Q, Zhang M, Quan P, et al. C-reactive protein and risk of breast cancer: A systematic review and meta-analysis [Internet]. Sci Rep. 2015;5(1):10508. DOI: 10.1038/srep10508
50. Kiesel L, Kohl A. Role of the RANK/RANKL pathway in breast cancer [Internet]. Maturitas. 2016;86:10-6. DOI: 10.1016/j.maturitas.2016.01.001
51. Bernhard VR, Faveri M, Santos MS, Gomes MDCM, Batitucci RG, Tanaka CJ, et al. Subgingival microbial profile of women with breast cancer: a cross-sectional study [Internet]. Appl Cancer Res. 2019;39(1):13. DOI: 10.1186/s41241-019-0082-3
52. Van Der Merwe M, Van Niekerk G, Botha A, Engelbrecht AM. The onco-immunological implications of Fusobacterium nucleatum in breast cancer [Internet]. Immunology Letters. 2021;232:60-6. DOI: 10.1016/j.imlet.2021.02.007
53. Little A, Tangney M, Tunney MM, Buckley NE. Fusobacterium nucleatum : a novel immune modulator in breast cancer? [Internet]. Expert Rev Mol Med. 2023;25:e15. DOI: 10.1017/erm.2023.9
54. Guo X, Yu K, Huang R. The ways Fusobacterium nucleatum translocate to breast tissue and contribute to breast cancer development [Internet]. Molecular Oral Microbiology. 2024;39(1):1-11. DOI: 10.1111/omi.12446
55. Sayehmiri F, Sayehmiri K, Asadollahi K, Soroush S, Bogdanovic L, Jalilian FA, et al. The prevalence rate of Porphyromonas gingivalis and its association with cancer: A systematic review and meta-analysis [Internet]. Int J Immunopathol Pharmacol. 2015;28(2):160-7. DOI: 10.1177/0394632015586144
56. Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, Fine DH, et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions [Internet]. Journal of Periodontology. 2018;89(S1). DOI: 10.1002/JPER.17-0721
Conflicts of interest
No conflicts of interests are declared. The authors declare that no grants were involved in this work.
Contribution of the authors
Conceptualization: Fiki Muhammad Ridho, Ridwan Alfatah.
Data curation: Fiki Muhammad Ridho, Alfi Syahri, Anis Irmawati.
Formal analysis:
Fiki Muhammad Ridho, Siska Maulidina Cahyani, Ridwan Alfatah.
Methodology:
Fiki Muhammad Ridho, Siska Maulidina Cahyani, Alfi Syahri, Anis
Irmawati.
Project administration: Fiki Muhammad Ridho.
Software:
Fiki Muhammad Ridho, Siska Maulidina Cahyani, Ridwan Alfatah.
Supervision: Anis Irmawati.
Writing - original draft:
Fiki Muhammad Ridho, Siska Maulidina Cahyani, Ridwan Alfatah, Alfi
Syahri.
Writing - review and editing:
Fiki Muhammad Ridho, Siska Maulidina Cahyani, Ridwan Alfatah, Alfi
Syahri, Anis Irmawati.
Data availability
Supplementary file: Research results. Word 2016. Available from: https://revmedmilitar.sld.cu/index.php/mil/libraryFiles/downloadPublic/62