Research Article
Association between serum progesterone concentration on the day before frozen embryo transfer and pregnancy outcomes
Asociación entre la concentración sérica de progesterona el día anterior a la transferencia de embriones congelados y los resultados del embarazo
Thi Hang Doan1 https://orcid.org/0000-0002-2972-5289
Quoc Thanh Trinh1 https://orcid.org/0009-0000-7264-548X
Minh Phuong Nguyen1 https://orcid.org/0000-0003-2933-172X
An Thien Trinh1 https://orcid.org/0000-0002-4047-5786
Hanh M. Pham2 https://orcid.org/0000-0002-8848-4665
The Son Trinh1 https://orcid.org/0000-0002-3807-9645
Tran Van Tuan1 https://orcid.org/0000-0002-5501-5723
Nguyen Ngoc Nhat1 https://orcid.org/0000-0003-3378-9290
1Vietnam Military Medical University. Military Institute of Clinical Embryology and Histology. Hanoi, Vietnam.
2Andrology and Fertility Hospital. Hanoi, Vietnam.
*Author for Correspondence. Email: trinhtheson@vmmu.edu.vn
ABSTRACT
Introduction: Progesterone is a key hormone linked to in vitro fertilisation outcomes, and serum progesterone is a significant marker before embryo transfer.
Objective: To evaluate the relationship between serum progesterone (P4) concentrations measured one day before frozen blastocyst transfer and pregnancy outcomes.
Methods: The prospective study included 276 frozen blastocyst transfer cycles. Endometrial preparation was performed using hormone replacement therapy (HRT), and luteal support was provided with 800 mg micronized vaginal progesterone and 20 mg oral dydrogesterone daily. Serum P4 was measured one day before embryo transfer. The positive hCG rate, clinical pregnancy rate, and live birth rate were evaluated.
Results: The live birth group had significantly lower mean P4 levels than the non-live birth group (13.1 vs 15.7 ng/mL, p = 0.0008). Clinical pregnancy and live birth rates were lower in the highest P4 tercile (>14.50 ng/mL) compared to lower terciles (<14.50 ng/mL). A receiver operating characteristic analysis showed serum P4 was a significant predictor of live birth, with an optimal cut-off of 14.75 ng/mL (44.8% sensitivity, 81.2% specificity).
Conclusions: In patients using our HRT protocol, higher serum progesterone levels on the day before embryo transfer were associated with reduced pregnancy and live birth rates.
Keywords: dydrogesterone; embryo transfer; hormone replacement therapy; progesterone.
RESUMEN
Introducción: La progesterona es una hormona clave en la fertilización in vitro y su concentración sérica es un marcador importante antes de la transferencia embrionaria.
Objetivo: Evaluar la relación entre los niveles séricos de progesterona (P4), medidos un día antes de la transferencia de blastocistos congelados y los resultados del embarazo.
Métodos: Estudio prospectivo que analizó 276 ciclos de transferencia de blastocistos congelados. La preparación endometrial se realizó mediante terapia de reemplazo hormonal (TRH), con soporte lúteo basado en 800 mg de progesterona vaginal micronizada y 20 mg de didrogesterona oral al día. Se midió la P4 sérica un día antes de la transferencia. Se evaluaron las tasas de hCG positiva, embarazo clínico y nacidos vivos.
Resultados: El grupo con nacidos vivos mostró niveles medios de P4 significativamente más bajos que el grupo sin nacidos vivos (13,1 vs. 15,7 ng/mL; p= 0,0008). Las tasas de embarazo clínico y nacidos vivos fueron menores en el tercil con mayor P4 (>14,50 ng/mL). El análisis ROC indicó que la P4 sérica predijo de forma significativa los nacidos vivos, con un punto de corte óptimo de 14,75 ng/mL (sensibilidad 44,8 %, especificidad 81,2 %).
Conclusión: En pacientes con el protocolo de TRH, niveles séricos elevados de progesterona el día previo a la transferencia se asociaron con menores tasas de embarazo clínico y nacidos vivos.
Palabras clave: didrogesterona; progesterona; terapia de reemplazo hormonal; transferencia de embriones.
Received: 23/07/2025
Approved: 03/11/2025
INTRODUCTION
In recent years, the utilisation of frozen embryo transfer (FET) has become increasingly popular in fertility centres worldwide, including Vietnam. FET cycles offer numerous advantages for couples struggling with infertility. During these cycles, luteal phase support has a critical role in ensuring successful implantation and improving the pregnancy rate. In particular, in hormonal replacement therapy (HRT) cycles where the natural corpus luteum is absent due to the use of exogenous hormone to prepare the endometrium, progesterone supplementation during the luteal phase has been associated with increasing live birth rate by using micronised vaginal progesterone (MVP) or oral dydrogesterone, which are equally well tolerated and have the same safety profile.(1)
Numerous studies have explored luteal phase support approaches in FET cycles. One such approach involves the combined use of MVP and oral dydrogesterone. This combination aims to optimise drug absorption and pharmacodynamics, considering the variations in absorbability and metabolic rates among individuals. Vuong LN et al.(2) conducted a prospective cohort study comparing the combined regimen with MVP alone and found a substantial difference in live birth rates between the two groups.
The efficacy of the combined regimen cannot be solely assessed by measuring serum P4 levels. It is important to acknowledge that progesterone intake may not be accurately reflected in serum P4 levels. However, previous studies have established a strong association between serum P4 concentration and pregnancy rate and live birth rate.(3,4,5) Hence, monitoring serum progesterone levels is necessary in HRT FET cycles.
Therefore, the study aims to assess the relationship between serum P4 concentration measured one day before frozen blastocyst transfer and pregnancy outcomes.
METHODS
Study population
This prospective cohort study was carried out at the Military Institute of Clinical Embryology and Histology from December 2020 to December 2022. The study focuses on women who underwent endometrial preparation using HRT for FET. Eligible participants had an endometrial thickness ranging from 7-14 mm on the day of progesterone administration and had good quality frozen-thawed blastocysts available to transfer. Meanwhile, exclusion criteria comprised women undergoing oocyte or embryo donation cycles, experiencing recurrent pregnancy loss, or having anatomical abnormalities in the uterus or fallopian tubes. Women with fluid accumulation in the uterine cavity or serum progesterone concentration below five ng/mL one day prior to FET were also excluded.(6,7)
During the study period, 343 women were prepared with HRT and had good quality blastocysts to transfer. However, there were 67 participants excluded during the process due to withdrawing from the study or having exclusion criteria. Exclusion criteria include: endometrial thickness < 7 mm and > 14 mm; donor oocytes; recurrent pregnancy loss history; P4 < 5 ng/mL; and did not respond. Finally, 276 FET cycles from eligible women were included in this study, all of whom were provided informed consent after receiving a comprehensive explanation of the study’s purpose procedures (Fig. 1). The participants were categorised into two groups: Group I (n = 133) with the presence of a live birth and Group II (n = 143) with the absence of a live birth.
Variables
Analytic variables included: The female age, BMI, type of infertility number of retrieved oocytes, number of MII oocytes, fertilisation rate, endometrial thickness on P4 administration day and on the day of FET, and P4 concentration of the two groups were analysed descriptively. The female age, BMI, hCG positive, and the rate of clinical pregnancy, live birth and miscarriage of the three tercile groups were calculated.
Study design
Endometrial preparation and luteal phase support
All the participants in this study received HRT for endometrial preparation. Starting on the second and third days of the menstrual cycle, each woman received a daily dose of 4 – 12 mg estradiol valerate depending on their endometrial development (Progynova®, Bayer). After 12-15 days of estradiol administration, all women received a standardised protocol for luteal phase support. This included 800 mg MVP (Utrogestan®, Besins), 20 mg dydrogesterone (Duphaston®, Abbott) and 4 mg estradiol valerate daily. Embryo transfer was performed on the 6th day of progesterone administration. HRT was continued until the participants did a pregnancy test. In case of a positive pregnancy, estradiol valerate was continued until week 8, and progesterone was administered until week 12 of gestation.
Serum analysis and hormone measurement
On the morning of the 5th day of progesterone administration, which is one day before FET, a blood sample was collected between 4–6 hours after the participants took the last dose of progesterone supplementation. Serum progesterone concentration was measured using an electrochemiluminescence immunoassay (Cobas 8000, Roche–Hitachi, Germany).
Embryo thawing and morphology assessment
The thawing protocol was performed using Kitazato® VT602 thawing media (Kitazato, Japan). All vitrified day five embryos were thawed on day 6 of progesterone administration and transferred on the same day. The Istanbul Consensus Workshop on Embryo Assessment was used as the basis for the blastocysts grading.(8) The study encompassed solely those participants who possessed good-quality embryos eligible for transfer.
Pregnancy outcome measurements
A human chorionic gonadotrophin (hCG) test was administered 12 days after the frozen embryo transfer. A positive result was defined as a hCG concentration exceeding 25 IU/L. Clinical pregnancy was determined by the detection of a gestational sac via transvaginal ultrasound. Live birth was the complete expulsion or extraction from a woman of a product of fertilisation after 22 completed weeks of gestational age, which, after such separation, breathed or showed any other evidence of life. Miscarriage was defined as the loss of clinical pregnancy.(9)
Statistical analysis
IBM SPSS Statistics version 22.0 software (SPSS Inc., Chicago, IL, USA) was employed for conducting the statistical analysis. Given a p-value of ≤ 0.05, the statistical tests were confirmed as indicating statistical significance.
First, 276 cycles were divided into two groups in accordance with the presence or absence of a live birth. Then, the serum progesterone concentration measured one day prior to FET was stratified into tercile groups (T1, T2 and T3). Then all the categorical variables were compared by using the Chi-square test or Fisher’s exact test between groups while the continuous variables were compared by using the Student’s t-test, then the Tukey post hoc tests were used to determine which groups were significant different from others. A multivariate logistic regression analysis was executed to pinpoint the factors influencing live birth outcomes. The predictive capability of serum progesterone concentration on live birth rate was assessed by constructing the receiving operating characteristic (ROC) curve. After that, the area under the curve (AUC) was calculated to find the prognostic level and the optimal cut-off to predict the live birth rate was defined according to sensitivity and specificity.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Committee of Vietnam Military Medical University (No.1186/2020/VMMU-IRB). Informed consent was obtained by distributing the consent form and asking for acceptance with a signature from all participants involved in the study.
RESULTS
The mean age of the participants was 32.2 ± 4.4 years, and the mean BMI was 21.7 ± 2.5 kg/m2. The mean serum progesterone concentration on the day before embryo transfer was 14.5 ± 6.4 ng/mL. The rates of β-hCG-positive, clinical pregnancy, live birth and miscarriage were 57.6% (159/276), 52.5% (145/276), 48.2% (133/276) and 8.3% (12/145), respectively.
BMI, age, infertility type, number of retrieved oocytes, number of mature oocytes (MII), fertilisation rate and endometrial thickness (ET) on both the progesterone administration day and the transfer day were found to be similar between the two groups. However, the mean concentration of progesterone on the day before embryo transfer was significantly higher in Group II compared to Group I (15.7 ± 7.3 ng/mL vs 13.1 ± 4.9 ng/mL, p = 0.0008) (table 1).
The mean of age, BMI and miscarriage rate were found no significant difference among three groups. Meanwhile, the rate of hCG positive, clinical pregnancy and live birth rate of were statistically different among terciles. Further analysis showed a significant lower clinical pregnancy and live birth rate in the highest tercile group (T3:>14.50ng/mL) than the first two group (T1:<11.45ng/mL and T2:11.45-14.50ng/mL) (table 2).
Only one significant variable was found: the serum P4 concentration one day prior to FET (p = 0.001, OR: 0.93, 95% CI: 0.89 - 0.97) (table 3).
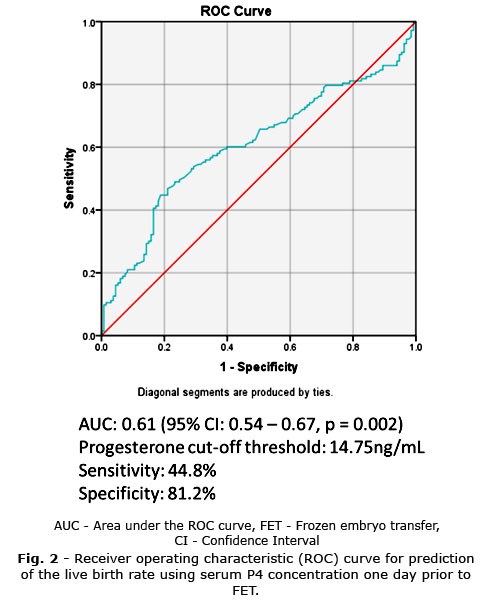
The ROC curve analysis showed an AUC of 0.61 (95% CI: 0.54-0.67, p = 0.002) for the serum progesterone concentration one day prior to FET, indicating a reasonably significant predictive value for the live birth rate. The optimal sensitivity and specificity were calculated, yielding a serum P4 cut-off of 14.75 ng/mL (sensitivity: 44.8%, specificity: 81.2%) (Fig. 2). The live birth rate was found to be significantly higher in women with serum P4 < 14.75 compared to those with serum P4 ≥ 14.75 ng/mL (57.8% vs 28.1%, p = 0.000). There was no significant difference in miscarriage rates between the two groups (5.3% vs 19.4%, p = 0.179).
DISCUSSION
The role of progesterone in endometrial maturation and its impact on implantation window synchrony may explain the observed relationship between P4 levels and pregnancy outcomes. Low progesterone levels can delay or impede endometrial maturation, while excessive progesterone levels may accelerate the endometrium development, which leads to asynchrony between the embryo and the endometrium.(10) Indeed, Thomsen L et al.(11) found an optimal range for the concentration of serum P4 in the early luteal phase, between 60-100 nmol/L (or 18.9-31.5 ng/mL); and the live birth rate in IVF treatment reduced significantly when the concentration of P4 was out of this range. Therefore, monitoring progesterone levels is crucial to predicting pregnancy outcomes and optimising luteal support for the individual woman.
The study findings highlighted the importance of progesterone in the success of FET cycles with HRT for endometrial preparation. The serum progesterone concentration on the day before embryo transfer was identified as a significant predictor of live birth outcomes.
The ROC curve shows that the serum P4 concentration had a suggestive predictive value for live birth rate, as indicated by an AUC value of 0.61. These findings agree with those in the previous studies that reported the predictive value of serum progesterone concentration for FET outcomes. Previous studies have shown similar AUC values for P4 concentration in predicting live birth rate, further supporting the notion that serum P4 is a valuable predictor of FET outcome.(10,12)
However, the optimal threshold of serum P4 levels on the day or one day prior to embryo transfer in FET cycles using a combination of MVP and oral dydrogesterone remains a controversial issue. The study performed by Kofinas JD et al.(13) concluded that serum progesterone levels > 20 ng/mL on the embryo transfer day were in association with decreased pregnancy rate and live birth rate. In addition, the prospective study by Alyasin A et al.(10) also demonstrated that serum progesterone concentrations > 32.5 ng/mL on embryo transfer day reduced live birth rate in HRT cycles. The P4 cut-off threshold in Alyasin A et al.(10) study was higher compared to other studies, including our study, because this study used both vaginal and intramuscular progesterone to luteal phase support.
On the other hand, some studies have reported an association between low progesterone levels before embryo transfer and a significant reduction in pregnancy outcomes. Gaggiotti-Marre S et al.(6) demonstrated progesterone levels ≤ 10.64 ng/mL on the day before embryo transfer, which resulted in a higher miscarriage rate and lower live birth rate, while high serum progesterone levels were associated with increased pregnancy outcomes. Other studies with HRT using vaginal progesterone administration have also indicated that P4 levels below ~ 10 ng/mL before embryo transfer or during early pregnancy have a detrimental effect on pregnancy outcomes.(14) Meanwhile, Neumann K et al.(15) study took a different approach as his team measured dydrogesterone and 20 α-dihydrogesterone serum levels in FET cycles using only oral dydrogesterone and resulted in the lower dydrogesterone plasma concentrations correlated with a decrease in ongoing pregnancy rate.(15) These contrasting findings may be attributed to the different luteal support protocols and progesterone administration routes used in the studies.
In this study, the combination of MVP and oral dydrogesterone for LPS is administered daily according to one of the most extensive prospective cohort studies investigating this combination.(2) Another study by Baldini GM et al.(16) also suggested 800 mg doses of MVP over 600 mg. The regimen used in the study might have influenced the minimum threshold of progesterone required for successful pregnancy because serum progesterone level only reflects the absorption of MVP but not dydrogesterone. As a result, the T1 group in this study, with a progesterone concentration < 11.45 ng/mL, had a similar live birth rate as the T2 group. This suggests that the minimum threshold of progesterone for pregnancy may be lower when using a combination of oral and vaginal progesterone compared to studies using vaginal progesterone alone.
However, there are some limitations to consider. The study uses a relatively small sample size, leading to the necessity of larger-cohort research to validate the relationship between serum P4 concentration and pregnancy outcomes. Moreover, there was a lack of control whether participants abstained from sexual intercourse during the luteal phase, which could affect progesterone levels after progesterone administration.(17)
This study highlights the significance of serum progesterone concentration one day prior to FET in HRT using a combination of MVP and dydrogesterone for luteal phase support. Higher progesterone levels were associated with a reduced live birth rate. Further research should be necessary to confirm these findings and determine the optimal threshold of progesterone for specific luteal phase support regimens.
Acknowledgements
The research team would like to express the sincerest gratitude to the Military Institute of Clinical Embryology and Histology, Vietnam Military Medical University, for their kind support during the data collection process.
BIBLIOGRAPHIC REFERENCES
1. Lorillon M, Robin G, Keller L, Cailliau E, Delcourt C, Simon V, et al. Is oral dydrogesterone equivalent to vaginal micronized progesterone for luteal phase support in women receiving oocyte donation? [Internet] Reproductive biology and endocrinology: RB&E. 2024;22(1):154. DOI: 10.1186/s12958-024-01322-7
2. Vuong LN, Pham TD, Le KT, Ly TT, Le HL, Nguyen DT, et al. Micronized progesterone plus dydrogesterone versus micronized progesterone alone for luteal phase support in frozen-thawed cycles (MIDRONE): a prospective cohort study [Internet]. Human Reproduction. 2021;36(7):1821-31. DOI: 10.1093/humrep/deab093
3. Alsbjerg B, Labarta E, Humaidan P. Serum progesterone levels on day of embryo transfer in frozen embryo transfer cycles—the truth lies in the detail [Internet]. Journal of Assisted Reproduction Genetics. 2020;37:2045-6. DOI: 10.1007/s10815-020-01851-1
4. Alur-Gupta S, Hopeman M, Berger DS, Barnhart KT, Senapati S, Gracia C. Measuring serum estradiol and progesterone one day prior to frozen embryo transfer improves live birth rates [Internet]. Fertility Research Practice. 2020;6(1):1-7. DOI: 10.1186/s40738-020-00075-2
5. Álvarez M, Gaggiotti-Marre S, Martínez F, Coll L, García S, González-Foruria I, et al. Individualised luteal phase support in artificially prepared frozen embryo transfer cycles based on serum progesterone levels: a prospective cohort study [Internet]. Human Reproduction. 2021;36(6):1552-60. DOI: 10.1093/humrep/deab031
6. Gaggiotti-Marre S, Martinez F, Coll L, Garcia S, Álvarez M, Parriego M, et al. Low serum progesterone the day prior to frozen embryo transfer of euploid embryos is associated with significant reduction in live birth rates [Internet]. Gynecological Endocrinology. 2019;35(5):439-42. DOI: 10.1080/09513590.2018.1534952
7. Volovsky M, Pakes C, Rozen G, Polyakov A. Do serum progesterone levels on day of embryo transfer influence pregnancy outcomes in artificial frozen-thaw cycles [Internet]. Journal of Assisted Reproduction Genetics. 2020;37:1129-35. DOI: 10.1007/s10815-020-01713-w
8. Coticchio G, Ahlström A, Arroyo G, Balaban B, Campbell A, De Los Santos MJ, et al. The Istanbul Consensus update: a revised ESHRE/ALPHA consensus on oocyte and embryo static and dynamic morphological assessment [Internet]. Reprod Biomed Online. 2025;50(6):104955. DOI: 10.1016/j.rbmo.2025.104955
9. Quenby S, Gallos ID, Dhillon-Smith RK, Podesek M, Stephenson MD, Fisher J, et al. Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss [Internet]. The Lancet. 2021;397(10285):1658-67. DOI: 10.1016/S0140-6736(21)00682-6
10. Alyasin A, Agha-Hosseini M, Kabirinasab M, Saeidi H, Nashtaei MS. Serum progesterone levels greater than 32.5 ng/ml on the day of embryo transfer are associated with lower live birth rate after artificial endometrial preparation: a prospective study [Internet]. Reproductive Biology Endocrinology. 2021;19:1-9. DOI: 10.1186/s12958-021-00703-6
11. Thomsen L, Kesmodel U, Erb K, Bungum L, Pedersen D, Hauge B, et al. The impact of luteal serum progesterone levels on live birth rates—a prospective study of 602 IVF/ICSI cycles [Internet]. Human Reproduction. 2018;33(8):1506-16. DOI: 10.1093/humrep/dey226
12. Ranisavljevic N, Huberlant S, Montagut M, Alonzo PM, Darné B, Languille S, et al. Low Luteal Serum Progesterone Levels Are Associated With Lower Ongoing Pregnancy and Live Birth Rates in ART: Systematic Review and Meta-Analyses. Frontiers in endocrinology. 2022;13:892753. DOI: 10.3389/fendo.2022.892753
13. Kofinas JD, Blakemore J, McCulloh DH, Grifo J. Serum progesterone levels greater than 20 ng/dl on day of embryo transfer are associated with lower live birth and higher pregnancy loss rates [Internet]. Journal of assisted reproduction genetics. 2015;32:1395-9. DOI: 10.1007/s10815-015-0546-7
14. Alsbjerg B, Thomsen L, Elbaek HO, Laursen R, Povlsen BB, Haahr T, et al. Progesterone levels on pregnancy test day after hormone replacement therapy-cryopreserved embryo transfer cycles and related reproductive outcomes [Internet]. Reproductive biomedicine online. 2018;37(5):641-7. DOI: 10.1016/j.rbmo.2018.08.022
15. Neumann K, Masuch A, Vonthein R, Depenbusch M, Schultze-Mosgau A, Eggersmann TK, et al. Dydrogesterone and 20alpha-dihydrodydrogesterone plasma levels on day of embryo transfer and clinical outcome in an anovulatory programmed frozen-thawed embryo transfer cycle: a prospective cohort study [Internet]. Hum Reprod. 2022;37(6):1183-93. DOI: 10.1093/humrep/deac045
16. Baldini GM, Mastrorocco A, Hatirnaz S, Malvasi A, Cazzato G, Cascardi E, et al. Evaluation of the ideal vaginal Progesterone effectiveness doses for luteal support in embryo thawing cycles after endometrial preparation without using the GnRh analogue [Internet]. Eur Rev Med Pharmacol Sci. 2023;27(5):2018-26. DOI: 10.26355/eurrev_202303_31568
17. Lawrenz B, Ata B, Fatemi HM. The good, the bad and the ugly of luteal phase stimulations. Reprod Biomed Online. 2024;49(6):104383. DOI: 10.1016/j.rbmo.2024.104383
Conflict of interest
The authors declare that they have no potential conflicts of interest relevant to this article.
Authorship contribution
Conceptualization: Hanh M. Pham, The Son Trinh.
Data curation: Thi Hang Doan, Quoc Thanh Trinh, An Thien Trinh, Minh Phuong Nguyen.
Formal analysis: Thi Hang Doan, The Son Trinh.
Methodology: Thi Hang Doan, Quoc Thanh Trinh, Hanh M. Pham.
Research: Thi Hang Doan, Quoc Thanh Trinh, Hanh M. Pham.
Supervision: The Son Trinh.
Drafting - Revision and editing: Thi Hang Doan, Minh Phuong Nguyen, The Son Trinh.
Drafting - Revision and final editing: Thi Hang Doan, Minh Phuong Nguyen, The Son Trinh.
Data Availability Statement
The database is available to readers upon request to the corresponding author at the following email address: trinhtheson@vmmu.edu.vn