Research Article
Evaluation of oocyte morphology in poor responders receiving testosterone before stimulation
Evaluación de la morfología ovocitaria en pacientes de baja respuesta que reciben testosterona antes de la estimulación
Thi Hang Doan1 https://orcid.org/0000-0002-2972-5289
The Son Trinh1 https://orcid.org/0000-0002-3807-9645
Tung Thanh Nguyen1 https://orcid.org/0000-0003-3790-9480
Minh Phuong Nguyen1 https://orcid.org/0000-0003-2933-172X
An Thien Trinh1 https://orcid.org/0000-0002-4047-5786
Van Tuan Tran1 https://orcid.org/0000-0002-5501-5723
Nguyen Ngoc Nhat1 https://orcid.org/0000-0003-3378-9290
Quoc Thanh Trinh1 https://orcid.org/0009-0000-7264-548X
1Vietnam Military Medical University. Military Institute of Clinical Embryology and Histology. Hanoi, Vietnam
*Author for Correspondence. Email: trinhquocthanh@vmmu.edu.vn
ABSTRACT
Introduction: Poor ovarian response is a significant challenge in assisted reproduction, and androgens have been associated with improved ovarian response.
Objective: To evaluate the impact of transdermal testosterone gel used prior to ovarian stimulation on oocyte quantity and quality in poor responders.
Methods: In this prospective study, 110 patients with poor ovarian response were randomized into two groups. Group 1 received transdermal testosterone gel for 21 days before ovarian stimulation, while group 2 (control) did not. Oocyte number, morphology, and maturity were assessed.
Results: The number of follicles ≥ 17 mm in group 1 was significantly higher than in group 2 (4.5 ± 1.7 vs. 2.6 ± 2.1, p = 0.00). Spherical, smooth polar bodies were more frequent in group 1 than in group 2 (75.7% vs. 66.1%; p = 0.02). The rate of metaphase II oocytes was significantly higher in group 1 compared to group 2 (89.6% vs. 81.9%, p = 0.02), as was the fertilization rate (84.1% vs. 74%, p=0.02).
Conclusions: Pretreatment with transdermal testosterone gel may improve both the quantity and quality of oocytes in poor responders undergoing in vitro fertilization.
Keywords: androgen; in vitro fertilization; oocytes; ovarian retrieval; testosterone.
RESUMEN
Introducción: La baja respuesta ovárica representa un desafío importante en la reproducción asistida y los andrógenos se han asociado con una mejora en la respuesta ovárica.
Objetivo: Evaluar el impacto del uso de gel de testosterona transdérmica antes de la estimulación ovárica, sobre la cantidad y calidad de los ovocitos en pacientes con baja respuesta ovárica.
Métodos: En este estudio prospectivo, 110 pacientes con baja respuesta ovárica fueron asignadas aleatoriamente a dos grupos. El grupo 1 recibió gel de testosterona transdérmica durante 21 días antes de la estimulación ovárica; el grupo 2 (control) no recibió testosterona. Se evaluaron el número, la morfología y la madurez de los ovocitos.
Resultados: El número de folículos ≥ 17 mm fue significativamente mayor en el grupo 1 que en el grupo 2 (4,5 ± 1,7 vs. 2,6 ± 2,1; p= 0,00). Los cuerpos polares esféricos y lisos fueron más frecuentes en el grupo 1 que en el grupo 2 (75,7 % vs. 66,1 %; p= 0,02). La tasa de ovocitos en metafase II fue significativamente mayor en el grupo 1 en comparación con el grupo 2 (89,6 % vs. 81,9 %; p= 0,02), al igual que la tasa de fecundación (84,1 % vs. 74,%; p= 0,.02).
Conclusiones: El tratamiento previo con gel de testosterona transdérmica podría mejorar tanto la cantidad como la calidad de los ovocitos en pacientes con baja respuesta ovárica sometidas a fertilización in vitro.
Palabras clave: andrógenos; fertilización in vitro; ovocitos; recuperación ovárica; testosterona.
Received: 11/07/2025
Approved: 06/11/2025
INTRODUCTION
Poor ovarian response (POR) is a significant challenge in assisted reproductive care, accounting for 9.0% to 24.0% of in vitro fertilization (IVF) cases.(1,2) Despite various ovarian stimulation regimens employed to address this issue, the treatment outcomes remain suboptimal. Currently, no treatment has demonstrated significant efficacy in improving poor response to ovarian stimulation.(3) However, Meldrum DR et al.(4) claimed that androgens are associated with increased ovarian response in his review.
Many meta-analysis and reviews still have different conclusions about the efficacy of transdermal testosterone prior to ovarian stimulation in IVF outcomes. Polyzos NP et al.’s(5) study and Subirá J et al.’s(6) study did not show a favourable result in the testosterone administration group. However, Sharma N et al.(7) observed a beneficial effect of androgen in IVF patients with poor ovarian response to gonadotrophin stimulation. The authors demonstrated improvements in ovarian response and outcomes with androgen supplementation, supporting the use of androgens as a pre-treatment strategy. Esparza M et al.(8)’s study suggested the same result.
Moreover, there is still a lack of evidence regarding the use of transdermal testosterone gel for women with poor response due to diminished ovarian reserve in the Vietnam despite our previous prospective study.(9)
Therefore, this study aims to assess the efficacy of transdermal testosterone gel on oocytes in patients with poor ovarian response prior to ovarian stimulation in IVF.
METHODS
Study design
In this study, 110 participants with POR voluntarily enrolled. It was conducted at the Military Institute of Clinical Embryology and Histology in Hanoi, Vietnam, from January 2020 to April 2021 following approval from the Ethical Review Committee of Vietnam Military Medical University. Each participant was provided with detailed information about the study and had written consent before participating.
Patients with a history of poor response, characterized by obtaining fewer than 3 oocytes with the standard ovarian stimulation regimen, abnormal ovarian reserve (with no more than 5 antral follicle counts and/or anti-Müllerian hormone levels ≤ 1.26 ng/mL), two cycles of unresponsive ovarian stimulation with the maximum dose, and who consented to participate in the study were selected. Additionally, patients with thyroid, liver, or kidney disease, a history of ovarian or pelvic surgery, uterine disease, involvement in third-party reproduction, or those who did not provide consent were excluded from the study.
The participants were randomly assigned to two groups: the first group consisted of patients who received transdermal testosterone gel (AndroGel® 1%, 5 g, Besins Healthcare, Brussel) 21 days before ovarian stimulation. These patients applied a quarter of an AndroGel® pack (equivalent to 12.5 mg testosterone) only to healthy, normal skin on the abdomen, shoulders, or upper arms. They were advised to apply the gel in the evening and after showering. The second group, serving as the control group, comprised patients who did not receive AndroGel® before ovarian stimulation.
Study population
Applying the formula for sample size calculation for testing the means of two groups:
n: Minimum sample size of each group
Z1-α/2: Confidence coefficient, corresponding to a 95% confidence level (α = 0,05) = 1,96
Z
SD1: Standard deviation of the mean number of oocytes in the group using AndroGel
SD2: Mean number of oocytes per patient in the group using AndroGel®
m1: Mean number of oocytes per patient in the group using AndroGel®
m2: Mean number of oocytes per patient in the control group
Based on the results from previous studies(6,7,8) regarding the mean number of oocytes, the values chosen were:
m1= 4,3; m2= 3,6; SD1= 2,1; SD2= 1,9
By substituting these values into the formula, the calculated sample size was n = 53. In this research, 55 participants were selected for the study group, and 55 participants were selected for the control group.
Oocytes Assessment
All patients underwent ovarian stimulation using a gonadotrophin-releasing hormone (GnRH) antagonist protocol. Once ultrasound examinations revealed the presence of at least two follicles measuring ≥ 17mm, human chorionic gonadotropin (hCG) was administered to trigger ovulation. Oocyte retrieval was performed using ultrasound-guided follicular aspiration approximately 36 hours after hCG injection. After incubated 3 hours, all oocytes were denudated and ready for inseminating. Meanwhile, the sperm samples underwent a rigorous processing technique. Initially, the spermatozoa were separated with density gradient centrifugation. Subsequently, a swim-up procedure was conducted to the post-washed sperm sample using G-IVF medium (Vitrolife). The prepared sperm samples were then used for cytoplasmic sperm injection (ICSI).
In terms of oocyte morphology and maturation, the following data were collected and analysed by at least two lab technicians before the oocytes were inseminated:
Number of retrieval oocytes and the nuclear maturation of those oocytes. Depending on the degree of nuclear maturity, an oocyte is divided into 3 stages. Germinal vesicle (GV) (in early stage I): the nucleus is still in the form of a spherical sac containing a large nuclear, no polar body (PB) in the perivitelline space (PVS). Stage metaphase I (MI): no presence of GV and no first polar body (PBI). Stage metaphase II (MII): presence of the PBI in the PVS.
Oocyte measurements: oocytes’ diameter, zona pellucida (ZP) thickness and ooplasm diameter (Fig. 1).
According to Ebner’s grading,(10) the polar body was classified according to the following characteristics: ovoid or round, smooth surface (A); ovoid or round, rough surface (B); fragmented (C); and large (D).
Assess the morphology of inclusions through the following grading: no inclusion (A); small inclusion body (B); one large inclusion or many small inclusions (C); and two large inclusions (D).
Vacuoles, well-defined transparent cavities inside ooplasm, were evaluated through the following categories: no vacuole (A); small vacuole (< 9 μm) (B); medium vacuole (9-18 μm) (C); and large vacuole (> 18 μm) (D).
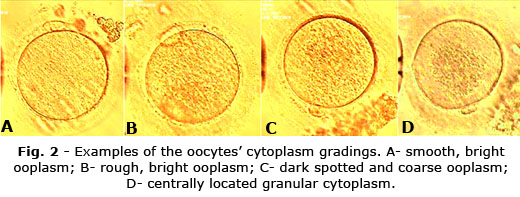
The granularity of the oocyte cytoplasm was assessed according to the following grading based on the description in Kahraman’s study: smooth, bright ooplasm (A); rough, bright ooplasm (B); dark spotted and coarse ooplasm (C); centrally located granular cytoplasm (D) (Fig. 2).(11)
Statistical analysis
IBM SPSS Statistics version 22.0 software (SPSS Inc., Chicago, IL, USA) was employed for conducting the statistical analysis. Differences in characteristics between the two cohorts were evaluated using Mann-Whitney U tests for the continuous variables and Chi-square tests or Fisher's exact test for the categorical variables. Given a p-value of ≤ 0.05, the statistical tests were confirmed as indicating statistical significance.
Ethical considerations
Informed consent was obtained by distributing the consent form and asking for acceptance with a signature from all participants involved in the study.
RESULTS
The difference in the mean age and average duration of infertility between the two groups was not statistically significant (p > 0.05). Similarly, there were no significant differences in the mean values of anti-Müllerian hormone (AMH), follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), and antral follicle count (AFC) when comparing the two study groups (p > 0.05). Sperm density and motility also did not show any significant differences between the groups (p > 0.05) (table 1).
In terms of follicle counts, the number of follicles ≥ 17 mm in group 1 was significantly higher than in group 2 (p < 0.05). The data also shows statistically significant differences between the two groups regarding the number of retrieved oocytes, day 3 embryos, transferred embryos, and frozen embryos (p < 0.05) (table 1).
The polar morphology of the two groups mostly consisted of spherical and smooth polar bodies and showed a significant difference between the two groups (p = 0.02). In group 1, 190 oocytes (75.7%) exhibited these characteristics; while in group 2, a lower number of 117 oocytes (66.1%). Additionally, the number of oocytes without polar bodies was significantly lower in group 1 compared to group 2 (10.3% vs 18.1%, p < 0.05) (table 2).
It was observed that cytoplasmic inclusions absence accounted for the most in group 1 with 179 oocytes (71.3%). The difference in the number of oocytes of the 2 groups in most ooplasmic inclusions categories was statistically significant (p < 0.05); whereas, in 2 inclusions category, there was no statistically significant difference in numbers with p = 0.95 (table 2).
Regarding vacuoles, the results indicated that there was a statistically significant difference between the two groups in terms of the presence of vacuoles in the oocyte cytoplasm. Group 1 had a higher proportion of oocytes without vacuoles (90.8% vs. 76.8%) and a lower number of oocytes with one small vacuole (6.5% vs. 15.3%) compared to group 2. Similarly, group 1 have lower of the number of oocytes with medium and large vacuoles than group 2, but there was no significant difference between two groups. Oocytes with smooth, bright cytoplasm accounted for the most in both groups with 174 oocytes (69.3%) in group 1 and 97 (54.8%) in group 2. Meanwhile, the number of oocytes whose cytoplasm was coarse granules, concentrated in the centre of the oocytes, accounted for the least of both groups, at 4.8% and 10.2%. The difference in the number of rough, bright cytoplasm oocytes of the two groups was not statistically significant (p = 0.91). In other cytoplasmic characteristics, the number of oocytes was significantly different statistically (p < 0.05) (table 2).
The results indicate that there were no significant differences in oocyte size, zona pellucida thickness, and oocyte cytoplasmic diameter between the two study groups. The number of MII oocytes accounted for the most in both groups with 225/251 (89.6%) in group 1 and 145/177 (89.9%) in group 2. The number of MII in group 1 was significantly higher than that of group 2 with p < 0.05. The number of GV oocytes was the least and the difference in the 2 groups was not statistically significant with p > 0.05 (table 3).
The number of fertilised oocytes in both groups was higher than the number of unfertilised oocytes, with 84.1% in group 1 and 74% in group 2. The fertilisation rate in group 1 was significantly higher than in group 2 (p < 0.05) (table 3).
DISCUSSION
The results of current study showed that there were similarities between two groups in age, infertility duration, hormonal testing, sperm count, sperm mobility, and three oocyte measurements. Nonetheless, there was significant differences in the number of large follicles (> 17 mm), retrieved oocytes, and embryos. This indicates that pre-treatment with transdermal testosterone gel might increase the chance of having higher number of follicles, leading to more oocytes, and more embryos, subsequently.
Not only increasing the quantity of oocytes, transdermal testosterone gel might also have an impact in oocyte quality. The maturation and fertilisation rate were both statistically higher in group with pre-treatment; furthermore, all the ‘good’ oocyte morphological indicators accounted higher percentage in treatment group than in the control group. Although, the correlation between oocyte morphological indicators with fertilisation outcome, or with embryo development is still controversial. Certain indicators may have no apparent effect, exert a limited influence, or negatively impact the outcomes of infertility treatment.(12,13,14,15)
Current results are similar to many studies, including descriptive prospective studies,(16,17,18,19) whereas, Sipe CS et al.’s(20) findings are opposed. However, the patients in Sipe CS et al.’s(20) study are advanced maternal age women, who are different from current study participants.
This study has several strengths, including its randomised controlled trial design, which minimize the confounding factors of participants. Additionally, all patients received the same IVF protocol, and the analysis was conducted in a single laboratory using consistent equipment.
There are some limitations to consider. The sample size was relatively small, and control group did not use a placebo gel. Therefore, more robust research with a placebo group is necessary to validate the efficacy of pre-treatment with Androgel®.
The observations show that the poor ovarian responders using Androgel® before ovarian stimulation had statistically higher number of the retrieval oocytes, better maturation rate, fertilisation rate, and better morphological features than the control group.
Acknowledgements
The research team would like to express the sincerest gratitude to the Military Institute of Clinical Embryology and Histology, Vietnam Military Medical University for their kind support during data collection process.
BIBLIOGRAPHIC REFERENCES
1. Guardo FD, Blockeel C, Vos MD, Palumbo M, Christoforidis N, Tournaye H, et al. Poor ovarian response and the possible role of natural and modified natural cycles [Internet]. Therapeutic advances in reproductive health. 2022; 16:1-8. DOI: 10.1177/26334941211062026
2. Lebovitz O, Haas J, Mor N, Zilberberg E, Aizer A, Kirshenbaum M, et al. Predicting IVF outcome in poor ovarian responders [Internet]. BMC Womens Health. 2022; 22(1):395. DOI: 10.1186/s12905-022-01964-y
3. Galatis D, Kalopita K, Grypiotis I, Flessas I, Kiriakopoulos N, Micha G, et al. Researching the Phenomenon of Poor Ovarian Responders and Management Strategies in IVF: A Narrative Review [Internet]. Acta Med Acad. 2022; 51(2):108-22. DOI: 10.5644/ama2006-124.379
4. Meldrum DR, Chang RJ, Giudice LC, Balasch J, Barbieri RL. Role of decreased androgens in the ovarian response to stimulation in older women [Internet]. Fertility sterility. 2013; 99(1):5-11. DOI: 10.1016/j.fertnstert.2012.10.011
5. Polyzos NP, Martinez F, Blockeel C, Gosalvez A, Fuente L, Pinborg A, et al. O-066 transdermal testosterone prior to ovarian stimulation for in vitro fertilization in women with poor ovarian response [Internet]. A multicenter multinational double-blind placebo-controlled randomized trial (the t-transport) [Internet]. Human Reproduction. 2023; 38(Supplement_1):dead093.080. DOI: 10.1093/humrep/dead093.080
6. Subirá J, Algaba A, Vázquez S, Taroncher DR, Mollá RG, Monzó FS, et al. Testosterone does not improve ovarian response in Bologna poor responders: a randomized controlled trial (testoprim) [Internet]. Reproductive BioMedicine Online. 2021; 43(3):466-74. DOI: 10.1016/j.rbmo.2021.05.021
7. Sharma N, Nayar KD. The effect of transdermal testosterone gel pretreatment on IVF outcomes in patients with poor ovarian reserve [Internet]. Journal of South Asian Federation of Obstetrics Gynaecology. 2023; 15(4):419-23. DOI: 10.5005/jp-journals-10006-2278
8. Esparza MEE, Ruvalcaba JLL, Salazar CGS, Salazar JC. Use of transdermal testosterone in women Poseidon IV group under high complexity assisted reproduction treatment [Internet]. Journal of IVF-Worldwide. 2024; 2(1):12-9. DOI:10.46989/001c.92149
9. Hoang QH, Ho HS, Do HT, Nguyen TV, Nguyen HP, Le MT. Therapeutic effect of prolonged testosterone pretreatment in women with poor ovarian response: A randomized control trial [Internet]. Reproductive Medicine Biology. 2021; 20(3):305-12. DOI: 10.1002/rmb2.12383
10. Ebner T, Yaman C, Moser M, Sommergruber M, Feichtinger O, Tews G. Prognostic value of first polar body morphology on fertilization rate and embryo quality in intracytoplasmic sperm injection [Internet]. Human Reproduction. 2000; 15(2):427-30. DOI: 10.1093/humrep/15.2.427
11. Kahraman S, Yakin K, Dönmez E, Samli H, Bahçe M, Cengiz G, et al. Relationship between granular cytoplasm of oocytes and pregnancy outcome following intracytoplasmic sperm injection [Internet]. Human Reproduction. 2000; 15(11):2390-3. DOI: 10.1093/humrep/15.11.2390
12. Nikiforov D, Grøndahl ML, Hreinsson J, Andersen CY. Human oocyte morphology and outcomes of infertility treatment: a systematic review [Internet]. Reproductive Sciences. 2022; 29(10): 2768-85. DOI: 10.1007/s43032-021-00723-y
13. Sciorio R, Tramontano L, Greco PF, Greco E. Morphological assessment of oocyte quality during assisted reproductive technology cycle [Internet]. JBRA Assist Reprod. 2024; 28(3):511-20. DOI: 10.5935/1518-0557.20240034
14. Fischer NM, Nguyen HV, Singh B, Baker VL, Segars JH Prognostic value of oocyte quality in assisted reproductive technology outcomes: a systematic review [Internet]. Reviews. 2021; 2(2):120-39. DOI: 10.1016/j.xfnr.2021.03.001
15. Balaban B, Keles I, Ebner T. Morphological assessment of oocyte quality [Internet]. Manual of Oocyte Retrieval Preparation in Human Assisted Reproduction. 2022; 85-97. DOI: 10.1017/9781108891646
16. Singh N, Parimalam P, Kumar S, Vanamail P. Role of transdermal testosterone gel pre-treatment on IVF outcome: a prospective randomized controlled trial with active control [Internet]. International Journal of Reproduction, Contraception, Obstetrics Gynecology. 2021; 10(9):3509-15. DOI: 10.18203/2320-1770.ijrcog20213476
17. Solernou R, Peralta S, Casals G, Guimera M, Solsona M, Borras A, et al. The Follicular Output Rate (FORT) as a method to evaluate transdermal testosterone efficacy in poor responders [Internet]. JBRA Assist Reprod. 2021; 25(2):229-34. DOI: 10.5935/1518-0557.20200086
18. Nayar K, Kaur G, Sanan S, Aggarwal S, Kant G. O-068 Transdermal testosterone gel (TTG) pre-treatment duration in improving ivf outcome in patients with poor prognosis (poseidon group 3 and 4): A randomised controlled trial [Internet]. Human Reproduction. 2023; 38(Supplement_1):dead093.082. DOI: 10.1093/humrep/dead093.082
19. Nayar K, Gupta S, Bhattacharya R, Mehra P, Mishra J, Kant G. P–612 Transdermal testosterone vs. Placebo (lubricant gel) pre-treatment in improving IVF outcomes in diminished ovarian reserve patients (Poseidon group 3 and 4): a randomised controlled trial [Internet]. Human Reproduction. 2021; 36(Supplement_1):deab130. 611. DOI: 10.1093/humrep/deab130.611
20. Sipe CS, Thomas MR, Stegmann BJ, Van VBJ. Effects of exogenous testosterone supplementation in gonadotrophin stimulated cycles [Internet]. Human Reproduction. 2010; 25(3):690-696. DOI: 10.1093/humrep/dep442
Conflict of interest
The authors declare that they have no potential conflicts of interest relevant to this article.
Authorship contribution
Conceptualization: Quoc Thanh Trinh, Thanh Tung Nguyen.
Data curation: Thi Hang Doan, The Son Trinh, Thanh Tung Nguyen, Minh Phuong Nguyen, An Thien Trinh, Van Tuan Tran.
Formal analysis: Thi Hang Doan, Quoc Thanh Trinh, Van Tuan Tran.
Methodology and Research: Thi Hang Doan, The Son Trinh, Minh Phuong Nguyen.
Supervision: Quoc Thanh Trinh.
Drafting - Revision and editing: Thi Hang Doan, Quoc Thanh Trinh, An Thien Trinh.
Data Availability Statement
The database is available to readers upon request to the corresponding author at the following email address: trinhquocthanh@vmmu.edu.vn