Research Article
Epidemiological and clinical characteristics of malaria patients in Khanh Hoa, Vietnam: The rise of Plasmodium malariae
Características epidemiológicas y clínicas de los pacientes con malaria en Khanh Hoa, Vietnam: Aumento de Plasmodium malariae
Quoc Long Dinh1 https://orcid.org/0009-0000-3514-1119
Ngoc Hieu Nguyen1 https://orcid.org/0000-0001-6091-3491
Hong Quang Huynh2 https://orcid.org/0000-0003-3895-7142
Truc Giang Truong Pham1 https://orcid.org/0009-0006-3800-907X
Duc Chinh Nguyen2 https://orcid.org/0009-0002-7692-2936
Manh Sieu Phu Tran1 https://orcid.org/0009-0002-6315-1319
Hue Van Thi Tran1* https://orcid.org/0009-0007-0677-2553
1University of Medicine and Pharmacy at Ho Chi Minh City. Ho Chi Minh City, Vietnam.
2Institute of Malariology, Parasitology, and Entomology Quy Nhon. Gia Lai, Vietnam.
*Author for correspondence. Email: huevan@ump.edu.vn
ABSTRACT
Background: In Vietnam, an unusual rise in P. malariae cases has been observed, accounting for a high proportion of malaria infections in Khanh Hoa province.
Objective: To describe the epidemiological and clinical characteristics of malaria cases caused by P. malariae in Khanh Hoa province, Vietnam, and to assess its recent emergence and distribution pattern.
Methods: A cross-sectional study was conducted in Khanh Vinh region, Khanh Hoa province, Vietnam. Confirmed malaria cases were collected from medical and laboratory records, including demographic, clinical, and parasitological data. Analyses identified trends and patterns of P. malariae infection.
Results: 93.68% of malaria infections were caused by P. malariae and 6.32% by P. vivax. Symptomatic P. malariae accounted for 96.63% of cases, with renal involvement (41.6%), splenomegaly (40.5%), and hepatomegaly (37.1%). The majority of infections occurred in the working-age population (64.2%). The Raglai ethnic group exhibited the highest prevalence (54.7%). The most affected occupation were farmer (72.6%) and students (18.9%). The highest infection rates were observed in Nam Khanh Vinh (36.8%) and Tay Khanh Vinh (37.9%), while P. vivax infections were reported solely in Bac Khanh Vinh and Nam Khanh Vinh.
Conclusions: P. malariae was the predominant species, largely associated with symptomatic infection and frequent renal, splenic, and hepatic involvement. Infections mainly affected the working-age population, with higher prevalence among the Raglai ethnic group, particularly farmers and students, and showed an uneven spatial distribution, with the highest burden in Nam Khanh Vinh and Tay Khanh Vinh.
Keywords: malaria; Plasmodium malariae; Vietnam.
RESUMEN
Antecedentes: En Vietnam, se observa un aumento de casos de P. Malariae. Representa una alta proporción de infecciones por malaria en la provincia de Khanh Hoa.
Objetivo: Describir características epidemiológicas y clínicas de casos de malaria por P. malariae en la provincia Khanh Hoa, Vietnam; evaluar su aparición y patrón de distribución.
Métodos: Estudio transversal. Se recopilaron los casos confirmados de malaria, de registros médicos, de laboratorio. Incluye datos demográficos, clínicos y parasitológicos. Los análisis identificaron tendencias y patrones de infección por P. malariae.
Resultados: La causa del 93,68 % de las infecciones fue P. Malariae; 6,32 % por P. vivax. P. malariae sintomática, 96,63 % de los casos; con afectación renal (41,6 %), esplenomegalia (40,5 %) y hepatomegalia (37,1 %). La mayoría de las infecciones fueron en población de edad laboral (64,2 %). El grupo étnico raglai tuvo prevalencia más alta (54,7 %); las ocupaciones más afectadas, agricultura (72,6 %) y estudiantes (18,9 %); tasas de infección más altas: En Nam Khanh Vinh (36,8 %) y Tay Khanh Vinh (37,9 %); las infecciones por P. vivax se registraron únicamente en Bac Khanh Vinh y Nam Khanh Vinh.
Conclusiones: P. malariae fue la especie predominante, asociada a infección sintomática y afectación renal, esplénica y hepática. Las infecciones afectaron a población en edad laboral, con mayor prevalencia entre el grupo étnico raglai, en particular agricultura y estudiantes; mostraron una distribución espacial desigual, con la mayor incidencia en Nam Khanh Vinh y Tay Khanh Vinh.
Palabras clave: malaria; Plasmodium malariae; Vietnam.
Received: 31/12/2025
Approved: 16/02/2026
INTRODUCTION
Malaria remains a critical global health challenge, with the World Health Organization (WHO) documenting an estimated 263 million cases and 597,000 deaths worldwide in 2023.(1) These data, reflecting an approximate 11-million increase in case incidence from the preceding year, highlights a troubling stalled momentum in reducing the disease burden, particularly in high-transmission regions. In contrast, elimination efforts have achieved substantial success, with the WHO certifying 44 countries and one territory as malaria-free by November 2024. Furthermore, 25 out of 83 endemic nations now report fewer than 10 annual cases, signifying a strategic contraction of the disease's footprint and validating the effectiveness of targeted interventions.(1,2)
Vietnam has made substantial progress in malaria control, with significant reductions in morbidity and mortality over the past three decades.(3) Nevertheless, during the early months of 2024, several provinces in the Central and Central Highlands regions experienced a localized resurgence in malaria incidence compared to the same period in 2023.(4) Most reported cases were caused by P. falciparum and P. vivax, the two dominant species in the region. Of particular epidemiological concern, however, is an outbreak in Khanh Hoa province that began in April 2023, distinguished by an unexpected predominance of P. malariae.(4)
Khanh Hoa province, located in the South Central Coast of Vietnam, features diverse geography comprising coastal plains, mountainous areas, and tropical forests. Khanh Vinh region, a mountainous subregion of the province covering approximately 1,165 km² with five communes, is inhabited predominantly by ethnic minority populations. The district remains socioeconomically disadvantaged, with limited transportation infrastructure and uneven healthcare coverage. Its hot and humid climate, dense forest cover, and numerous rivers and streams create highly favorable conditions for Anopheles mosquitoes to breed and sustain malaria transmission. As a result, Khanh Vinh region is recognized as one of the principal hotspots for malaria risk in Khanh Hoa province.
P. malariae infection has generally been underrecognized due to its relatively mild clinical manifestations and lower prevalence compared with P. falciparum and P. vivax. This species is characterized by the longest incubation period, ranging from 18 to 40 days, and a slow development cycle within red blood cells.(5) Consequently, both the clinical and laboratory features of P. malariae malaria remain insufficiently understood, largely owing to the limited number of studies compared with other human malaria species. Since 2023 and throughout the first half of 2024, however, an unusual increase in P. malariae mono-infections has been documented in Khanh Vinh region, Khanh Hoa province, Vietnam, accounting for approximately 48-65% of all confirmed malaria cases.(4,6)
This study aimed to describe the epidemiological and clinical characteristics of P. malariae malaria in Khanh Hoa province, Vietnam, and to assess its recent emergence and distribution.
METHODS
Study design
A cross-sectional study was conducted in Khanh Vinh region, Khanh Hoa province, central Vietnam, from November 2024 to August 2025.
Study subjects
The study population included both symptomatic and asymptomatic individuals who attended commune health centers in five communes of Khanh Vinh region, namely Tay Khanh Vinh, Dong Khanh Vinh, Nam Khanh Vinh, Bac Khanh Vinh, and Khanh Vinh. Participants were enrolled consecutively during the study period if they underwent malaria screening and provided peripheral blood samples. There was no restriction on age or sex.
Variables
Included sociodemographic characteristics, diagnostic methods, temporal distribution of infection, type of malaria parasite, and clinical features. Sociodemographic variables comprised sex, age, ethnicity, occupation, and place of residence. Diagnostic variables included malaria detection by Giemsa-stained blood smear microscopy and nested polymerase chain reaction (PCR). Temporal variables included the month of diagnosis, covering the period from November 2024 to August 2025. The type of malaria parasite was classified as P. malariae or P. vivax. Clinical variables included the presence of fever, mucocutaneous manifestations, hepatomegaly, splenomegaly, neurological symptoms, gastrointestinal disturbances, and signs of renal involvement.
Procedures
Peripheral blood samples were collected from all participants at their respective commune health centers. Thick and thin blood smears were prepared and stained with Giemsa for microscopic examination to detect malaria parasites. All microscopy-positive samples were subsequently transported to the Department of Medicine Laboratory, University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam, for molecular confirmation. Nested-PCR was performed to identify P. malariae according to standardized protocols. Sociodemographic information and clinical data were systematically recorded using a structured data collection form at the time of patient presentation.
A malaria case was defined as an individual with the presence of malaria parasites detected in peripheral blood by microscopy and subsequently confirmed as P. malariae infection by nested-PCR.
Data processing and statistical analysis
Data were entered and stored in Microsoft Excel 2021 and subsequently processed and analyzed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). A 95% confidence level was applied, and statistical significance was set at p < 0.05. Associations between age, ethnicity, occupation, residence, and sex were assessed using the Chi-squared test when more than 80% of the expected values were greater than 5; otherwise, Fisher’s exact test was applied. The Mann - Whitney U test was used to compare mean body mass index values between sexes.
Bioethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and relevant national regulations on biomedical research involving human subjects. Ethical approval was obtained from the Institute of Malariology, Parasitology, and Entomology Quy Nhon, Vietnam (Approval No. 981/VSR-GCN), prior to the initiation of the study.
All eligible participants were informed about the objectives, procedures, potential risks, and benefits of the study in a language they could understand. Written informed consent was obtained from all adult participants. For participants under 18 years of age, informed consent was obtained from parents or legal guardians, and assent was obtained from the participants whenever appropriate.
Participation in the study was entirely voluntary, and individuals were free to withdraw at any time without any impact on their access to medical care or treatment. To ensure confidentiality, all personal identifiers were removed from the dataset and replaced with unique study codes. Access to the data was restricted to authorized research personnel only.
Peripheral blood samples were collected following standard clinical and laboratory safety procedures to minimize discomfort and risk to participants. All patients diagnosed with malaria received appropriate treatment in accordance with the national malaria treatment guidelines of Vietnam. The study did not involve any experimental interventions beyond routine diagnostic procedures, and no financial incentives were provided for participation.
RESULTS
From November 2024 to August 2025, a total of 2,236 patients attended five commune health centers in Trung Khanh Vinh, Bac Khanh Vinh, Tay Khanh Vinh, Nam Khanh Vinh, and Khanh Vinh. Of these, 95 patients had blood samples positive for malaria parasites. Nested-PCR confirmed 89 (93.68%) cases of P. malariae monoinfection and 6 cases of P. vivax monoinfection, with no co-infections (table 1).
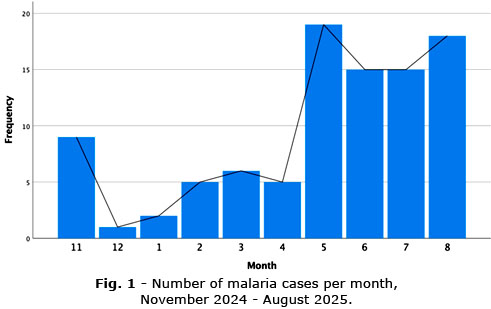
Malaria cases were recorded in all 10 months of the survey, with the highest numbers occurring between May and August, particularly in July (20% of cases), followed by May, June, and August (15.89 - 17.89%) (Fig. 1). The age group most affected was 18 - 60 years (68.4%, 65/95), and the majority of cases were male (74.7%, 71/95) (table 2).
The highest proportion of P. malariae infections was observed in the 16–18 (64.2%, 61/89) year age group, with most cases occurring in males (75.28%, 67/89). By ethnicity, the majority of infections were detected among Raglai (54.7%), followed by T’rin (14.7%) and Kinh (11.6%). Farmers (72.6%, 69/89) and students (18.9%, 18/89) represented the two occupational groups with the highest prevalence. Malaria cases were reported in all communes, with the highest proportions recorded in Nam Khanh Vinh (40%, 38/95) and Tay Khanh Vinh (37.9%, 36/95). Notably, P. vivax infections were restricted to Bac Khanh Vinh and Nam Khanh Vinh, whereas P. malariae infections occurred in four communes but were absent in Bac Khanh Vinh. The distribution of P. malariae and P. vivax infections was statistically significantly different between communes (p < 0.001) (table 2).
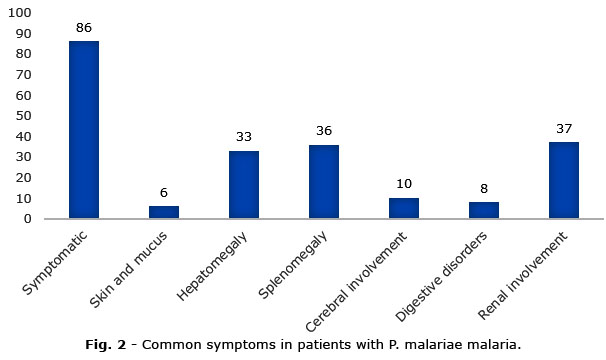
Of the 89 patients with P. malariae, 86 (96.6%) presented with clinical manifestations of malaria. Renal impairment was common, with elevated serum creatinine detected in 37 patients (41.6%), suggesting a high frequency of kidney involvement. Hepatomegaly and splenomegaly were also frequently observed, accounting for 37.1% and 40.5% of cases, respectively (Fig. 2).
DISCUSSION
In this study, microscopic examination of Giemsa-stained blood smears identified 95 samples with morphological features consistent with P. malariae. However, nested PCR analysis confirmed only 89 samples as P. malariae and identified 6 samples as P. vivax. This discrepancy observed in current study may be attributable to the morphological similarity of the trophozoite stages of P. malariae and P. vivax, highlighting that the accuracy of smear-based parasite identification largely depends on the skill and experience of local technicians. Therefore, this method has considerable limitations. The findings of this study demonstrate that molecular biology methods provide robust evidence for the accurate identification of malaria species, owing to their high sensitivity in detecting parasites at very low levels of parasitemia (as few as 1–5 parasites/µL of blood), which are often undetectable by microscopy. Previous studies conducted in Africa, Southeast Asia, and Brazil have also confirmed the superior diagnostic performance of PCR methods for detecting P. malariae.(7,8,9) For malaria prevention, diagnosis, and treatment, molecular biology techniques should be applied to ensure the accuracy of malaria species detection to help use the right treatment regimen as recommended by WHO.
Historically, P. malariae infections have been considered rare in malaria-endemic regions of Vietnam. However, since 2023, Khanh Vinh region in Khanh Hoa province has experienced an outbreak in which P. malariae emerged as the predominant species. P. malariae accounted for 46.1% of confirmed cases, with a peak in July 2024.(4) The findings of the present study are consistent with these observations, demonstrating a similar seasonal pattern, with case numbers increasing from May to August 2025 and peaking in July. This temporal trend corresponds with the rainy season in Khanh Vinh region (May - October), when dense vegetation provides favorable ecological conditions for the proliferation of Anopheles breeding sites, thereby amplifying malaria transmission risk.
Spatially, P. malariae infections were concentrated in four communes Nam Khanh Vinh, Tay Khanh Vinh, Trung Khanh Vinh, and Khanh Vinh of which Tay Khanh Vinh and Nam Khanh Vinh recorded the highest prevalence. These findings align with earlier reports documenting Khanh Thuong (now Tay Khanh Vinh) and Son Thai (now Nam Khanh Vinh) as the most affected localities.(4) By contrast, Bac Khanh Vinh commune reported only P. vivax infections. This pattern may reflect the historical predominance of P. vivax in Khanh Hoa, with relapses mediated by hypnozoites contributing to its persistence during the outbreak.(10) The majority of cases occurred in the working-age population, particularly among farmer (72.6%) and students (18.9%). Farm workers frequently engage in forest-related activities and overnight stays in fields, thereby increasing their exposure to Anopheles vectors. Attending semi-boarding schools in proximity to forested areas and commuting across fields or forest edges at dawn and dusk-the periods of highest Anopheles activity-exposes students to an increased risk of malaria infection. Moreover, the predominance of ethnic minority populations in these communes, coupled with limited awareness and uptake of preventive measures, may further exacerbate infections. Taken together, the findings of this study on the epidemiological profile of P. malariae are concordant with previous reports from the Central and Central Highland regions of Vietnam, underscoring the need for strengthened surveillance and targeted control measures in these high-risk populations.
The results of this study indicate that the vast majority of P. malariae infected patients were symptomatic (96.63%), with fever, hepatomegaly, and splenomegaly being the most common clinical manifestations. Notably, 37 of 89 patients exhibited signs of renal involvement, a characteristic complication of P. malariae infection. This observation is consistent with the spectrum of complications reported for P. malariae, including splenomegaly, high fever, seizures, anemia, and in particular immune complex - mediated glomerulonephritis. Several investigators have reported the strong association between P. malariae infection and renal pathology.(11) Hendrikse RG et al.(12) described clinicopathological features of P. malariae associated infection and suggested that immune complex deposition can induce structural glomerular damage, while Dixon FJ(13) demonstrated immune complex deposition in the kidneys of patients with nephrotic syndrome linked to P. Malariae.
From an epidemiological perspective, all P. malariae cases identified in this study were autochthonous to Khanh Vinh region. However, the classification of indigenous versus imported infections presents a major challenge due to the unusually long incubation and latency periods of P. malariae (16-59 days).(14) This significantly complicates malaria surveillance and elimination efforts, particularly in tracing the most likely site of acquisition through travel history. For P. malariae infections, expanding the recall period for travel history investigations beyond the conventional 14 days is essential to accurately identify transmission foci and to optimize the effectiveness of targeted control interventions.
In line with the study objective, this study describes the epidemiological and clinical characteristics of malaria caused by Plasmodium malariae in Khanh Hoa province, Vietnam. P. malariae was the predominant species, largely associated with symptomatic infection and frequent renal, splenic, and hepatic involvement. Infections mainly affected the working-age population, with higher prevalence among the Raglai ethnic group, particularly farmers and students, and showed an uneven spatial distribution, with the highest burden in Nam Khanh Vinh and Tay Khanh Vinh.
P. malariae was the predominant species, largely associated with symptomatic infection and frequent renal, splenic, and hepatic involvement. Infections mainly affected the working-age population, with higher prevalence among the Raglai ethnic group, particularly farmers and students, and showed an uneven spatial distribution, with the highest burden in Nam Khanh Vinh and Tay Khanh Vinh.
Acknowledgements
The authors wish to thank the University of Medicine and Pharmacy at Ho Chi Minh City and Institute of Malariology, Parasitology, and Entomology Quy Nhon, Vietnam for their valuable support and contributions to this study.
BIBLIOGRAPHIC REFERENCES
1. WHO. WHO world malaria report 2024: Addressing inequity in the global malaria response [Internet]. Geneva: WHO; 2025. [access: 10/12/2025]. Available from: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2024
2. Venkatesan P. The 2023 WHO World malaria report [Internet]. The Lancet Microbe. 2024 [access: 10/12/2025]; 5(3):e214. Available from: https://www.thelancet.com/journals/lanmic/article/PIIS2666-5247(24)00016-8/fulltext
3. Võ TC, Lê HG, Kang J-M, Naw H, Fan C-K, Trinh NTM, et al. Molecular surveillance of malaria in the Central Highlands, Vietnam [Internet]. Parasitology International. 2021; 83:102374. DOI: 10.1016/j.parint.2021.102374
4. Khanh CV, Lê HG, Võ TC, Quang NX, Nguyen DV, Dung NCT, et al. Unprecedented large outbreak of Plasmodium malariae malaria in Vietnam: epidemiological and clinical perspectives [Internet]. Emerging Microbes & Infections. 2025; 14(1):2432359. DOI: 10.1080/22221751.2024.2432359
5. McKenzie FE, Jeffery GM, Collins WE. Plasmodium malariae blood-stage dynamics [Internet]. The Journal of Parasitology. 2001; 87(3):626–37. DOI: 10.1645/0022-3395(2001)087[0626:PMBSD]2.0.CO;2
6. Dũng NCT, Hoà ĐV, Hào ĐV, Lê BTD, Sơn ND, Thoa NT, et al. Một số đặc điểm dịch tễ, lâm sàng, cận lâm sàng trường hợp bệnh sốt rét hiếm gặp do Plasmodium malariae tại huyện Khánh Vĩnh, tỉnh Khánh Hoà, năm 2023 [Internet]. Tạp chí Y học Dự phòng. 2024;34(5 Phụ bản):30–6. DOI: https://doi.org/10.51403/0868-2836/2024/1856
7. Snounou G, Pinheiro L, Gonçalves A, Fonseca L, Dias F, Brown KN, et al. The importance of sensitive detection of malaria parasites in the human and insect hosts in epidemiological studies, as shown by the analysis of field samples from Guinea Bissau [Internet]. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1993;87(6):649–53. DOI: 10.1016/0035-9203(93)90274-T
8. Rubio JM, Benito A, Roche J, Berzosa PJ, Garcia ML, Mico M, et al. Semi-nested, multiplex polymerase chain reaction for detection of human malaria parasites and evidence of Plasmodium vivax infection in Equatorial Guinea [Internet]. The American Journal of Tropical Medicine and Hygiene. 1999;60(2):183–7. DOI: 10.1016/0035-9203(93)90274-T
9. Walker-Abbey A, Djokam RRT, Eno A, Leke RFG, Titanji VPK, Fogako J, et al. Malaria in pregnant Cameroonian women: the effect of age and gravidity on submicroscopic and mixed-species infections and multiple parasite genotypes [Internet]. The American Journal of Tropical Medicine and Hygiene. 2005 [access: 10/12/2025];72(3):229–35. Available from: https://d1wqtxts1xzle7.cloudfront.net/42287542/229-libre.pdf?1454844658
10. Tam LT, Thinkhamrop K, Suttiprapa S, Clements ACA, Wangdi K, Suwannatrai AT. Bayesian spatio-temporal modelling of environmental, climatic, and socio-economic influences on malaria in Central Vietnam [Internet]. Malaria Journal. 2024 [access: 12/12/2025];23(1):258. Available from: https://link.springer.com/article/10.1186/s12936-024-05074-y
11. Warren M, Collins WE, Jeffery GM, Skinner JC. The seroepidemiology of malaria in Middle America. II. Studies on the Pacific coast of Costa Rica [Internet]. The American Journal of Tropical Medicine and Hygiene. 1975 [access: 12/12/2025];24(5):749–54. Available from: https://europepmc.org/article/med/1190364
12. Hendrickse RG, Adeniyi A. Quartan malarial nephrotic syndrome in children [Internet]. Kidney International. 1979;16(1):64–74. DOI: 10.1038/ki.1979.103
13. Dixon FJ. Comments on immunopathology [Internet]. Military Medicine. 1966; 131(suppl_9):1233–4. DOI: 10.1093/milmed/131.suppl_9.1233
14. Collins WE, Jeffery GM. Plasmodium malariae: parasite and disease [Internet]. Clinical Microbiology Reviews. 2007;20(4):579–92. DOI: 10.1128/cmr.00027-07
Conflict of interests
The authors declare that they have no competing interests.
Financial information
None.
Autorship contribution
Conceptualization: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran.
Data curation: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran.
Formal Analysis: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran, Hong Quang Huynh, Truc Giang Truong Pham, Duc Chinh Nguyen, Manh Sieu Phu Tran.
Research: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran.
Methodology: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran.
Project Administration: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran.
Resources: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran.
Supervision: Hue Van Thi Tran.
Validation: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran.
Writing - original draft: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran, Hong Quang Huynh, Truc Giang Truong Pham, Duc Chinh Nguyen, Manh Sieu Phu Tran.
Writing - Review & editing: Quoc Long Dinh, Ngoc Hieu Nguyen, Hue Van Thi Tran, Hong Quang Huynh, Truc Giang Truong Pham, Duc Chinh Nguyen, Manh Sieu Phu Tran.
Data availability
All data generated or analyzed in this study are contained within this published article. Additional information or supplementary materials related to the case reports can be obtained from the corresponding author upon reasonable request.