Case Presentation
Multiple and recurrent pilomatricoma in a pediatric patient
Pilomatrixoma múltiple y recurrente en un paciente pediátrico
Ariana Alexandra Campos Castillo1 https://orcid.org/0009-0008-3711-2432
Fabiola Fernanda Saravia Yataco1https://orcid.org/0009-0008-5469-7399
Víctor Fernando Maximiliano Vargas Uribe2 https://orcid.org/0009-0000-7086-7054
José Salvador-Carrillo1 https://orcid.org/0000-0001-7076-6093
Johan Espino-Ortiz3* https://orcid.org/0000-0003-0447-5794
Cindy Elizabeth Alcarraz Molina4 https://orcid.org/0000-0001-8488-8171
1Universidad Privada San Juan Bautista. Escuela Profesional de Medicina Humana. Chincha, Perú.
2Hospital Nacional San José de Chincha. Chincha, Perú.
3Universidad Privada San Juan Bautista. Escuela Profesional de Medicina Humana. Lima, Perú.
4Instituto Nacional de Enfermedades Neoplásicas. Lima, Perú.
*Correspondence Author. Email: johan.espino.297@gmail.com
ABSTRACT
Introduction: Pilomatricoma is a rare, benign skin tumor, with an estimated frequency of 1% among all skin tumors. It primarily affects the head and neck region, particularly in the pediatric population. While multiple pilomatricomas are uncommon and represent 0.7–3% of all cases, recurrent ones are even rarer and require special attention when managing this benign skin tumor.
Objective: To report a pediatric case of multiple and recurrent pilomatricomas, emphasizing its clinical characteristics diagnostic challenges, and therapeutic decisions.
Clinical Case: A 12-year-old male patient with multiple pilomatricomas since the age of six, who had previously undergone five surgical excisions. Currently, new tumors have emerged on his neck and thigh, steadily increasing in size. The lesions were subcutaneous, mobile, and non-painful, with no associated systemic symptoms or neurological conditions. Pathological examination and soft tissue ultrasonography confirmed the diagnosis of multiple and recurrent pilomatricoma, and a new surgical intervention was scheduled.
Conclusion: The patient developed more than seven tumors over a six-year period—a pattern uncommon in published pediatric cohorts. Recognizing the specific characteristics of multiple and recurrent pilomatricomas in pediatric patients is essential for accurate and timely diagnosis.
Keywords: diagnosis; pediatric; pilomatricoma; recurrence; skin neoplasms.
RESUMEN
Introducción: El pilomatrixoma es un tumor cutáneo benigno poco frecuente, que afecta sobre todo la región de la cabeza y el cuello. Las formas múltiples son raras y representan entre el 0,7 % y el 3 % de los casos, mientras que la recurrencia es aún menos común y plantea retos en el manejo clínico.
Objetivo: Reportar un caso pediátrico de lesiones múltiples y recurrentes, con énfasis en sus características clínicas, dificultades diagnósticas y decisiones terapéuticas.
Caso Clínico: Paciente varón de 12 años con antecedentes de múltiples lesiones desde los seis años, sometido a cinco exéresis quirúrgicas previas. En la evaluación actual presenta nuevos tumores en cuello y muslo, con crecimiento progresivo. Las lesiones eran subcutáneas, móviles y no dolorosas, sin síntomas sistémicos ni trastornos neurológicos asociados. El estudio anatomopatológico y la ecografía de partes blandas confirmaron el diagnóstico, por lo que se programó una nueva intervención quirúrgica.
Conclusión: El paciente desarrolló más de siete lesiones en un periodo de seis años, un patrón poco descrito en cohortes pediátricas. Reconocer estas formas múltiples y recurrentes en población pediátrica permite un diagnóstico oportuno y orienta el manejo adecuado.
Palabras clave: diagnóstico; neoplasia cutánea; pediatría; pilomatricoma; recurrencia.
Received: 25/12/2025
Approved: 30/04/2026
INTRODUCTION
Pilomatricoma (PM) is an uncommon benign cutaneous tumor derived from the hair follicle matrix, with a higher prevalence in children and adolescents. It accounts for approximately 1% of all benign skin tumors and most frequently affects the head and neck region.(1) Despite being well characterized, it remains underdiagnosed due to its variable presentation and overlap with other subcutaneous lesions.(2,3)
In contrast, multiple pilomatricoma (MPM) is a rare presentation, reported in a small proportion of cases, ranging from 0.7% to 3% of all PM cases. It is defined by the presence of two or more lesions and may follow a progressive course with the development of new nodules over time.(4,5) Additionally, its potential association with genetic syndromes or alterations in follicular matrix regulation has been highlighted. These features distinguish MPM from the typical solitary pattern and increase its clinical relevance.(4,6)
Diagnosis is primarily based on clinical evaluation and supported by imaging findings.(7) Ultrasound has proven useful in identifying calcified nodules, improving preoperative assessment, and aiding in atypical cases. However, histopathological examination remains the gold standard for confirmation, characterized by the presence of basaloid cells, ghost cells, and calcification.(2,7)
Although PM generally has a favorable prognosis and surgical excision is curative in most cases,(8) recurrence has been associated with incomplete excision. In contrast, in MPM, the development of lesions in different anatomical regions suggests a multifocal process rather than true recurrence, which has important implications for follow-up and clinical management.(6,8)
The current literature on MPM remains limited, with most reports involving pediatric patients who develop multiple lesions progressively over time. This gap highlights the importance of reporting additional cases to improve recognition and understanding of its clinical behavior.(4,6,8)
The case of a pediatric patient with progressive development of multiple lesions over several years is presented, consistent with MPM, emphasizing its clinical course and the need for long-term follow-up.
CLINICAL CASE
A 12-year-old Peruvian male presented to a healthcare facility with a history of MPM since age six. Prior to this visit, he had undergone five surgical excisions for these lesions, with no significant family history.
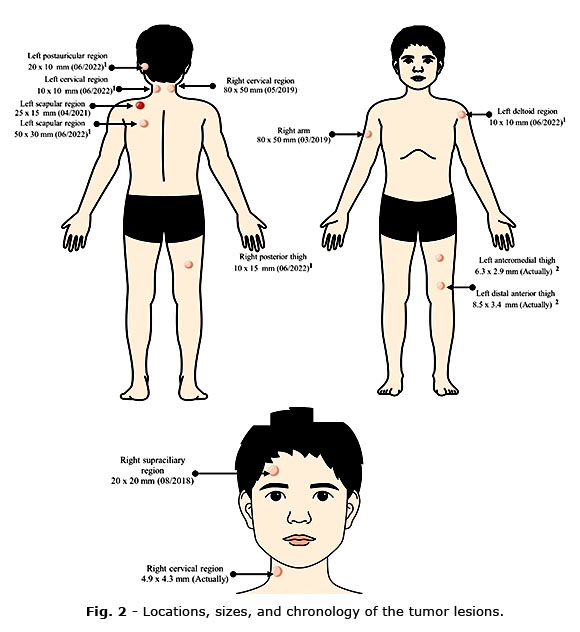
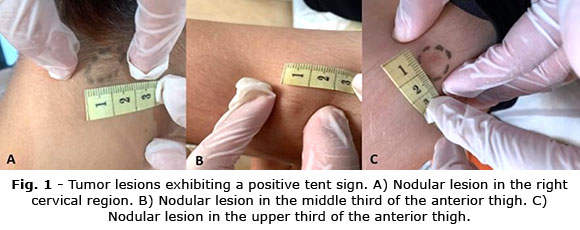
On examination, several new tumors were identified on the neck and left thigh, with an increase in size. The patient reported no associated systemic or neurological symptoms. The lesions were subcutaneous, mobile, and non-painful on palpation. A tumor measuring approximately 20 mm in diameter was identified in the right cervical region, along with two lesions measuring 10 mm in the left thigh. A positive tent sign supported the clinical suspicion of PM, as described in the literature (Fig. 1).
In previous years, the patient underwent surgical excision of tumors in the left retroauricular region, left deltoid, left scapular region, left cervical region, and posterior right thigh. These procedures achieved complete removal of the lesions, and histopathological examination confirmed PM. Figure 2 shows the sequence of tumor appearance.
Histopathological evaluation of a right supraciliary lesion excised in a previous procedure revealed a 2 × 1.8 cm tissue fragment with a grayish appearance and soft consistency on sectioning. Microscopic findings were consistent with Malherbe’s calcifying epithelioma.
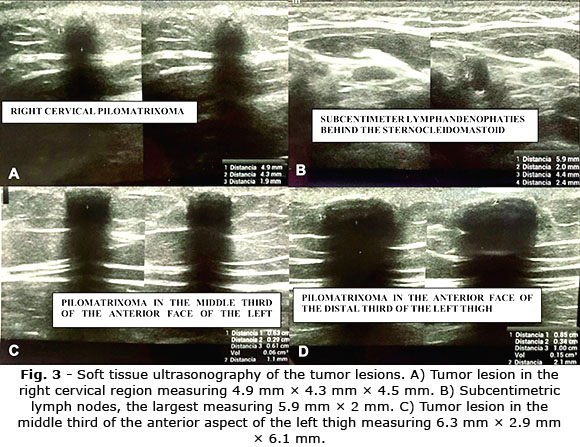
Ultrasonography of the soft tissues in the right cervical region showed an oval, solid-appearing nodule with calcified content, surrounded by a thin hypoechoic halo and minimal peripheral vascularization (4.9 × 4.3 × 4.5 mm). Similar nodules were identified in the middle and distal thirds of the anterior left thigh (6.3 × 2.9 × 6.1 mm and 8.5 × 3.4 × 10 mm, respectively). Subcentimetric lymph nodes were also noted posterior to the sternocleidomastoid muscle (Fig. 3).
A neurological evaluation of the motor system—including muscle trophism, osteotendinous reflexes, gait, strength, and tone—revealed no abnormalities. Based on these results and the patient's history, he was referred to the surgical department for planned excision with 1 – 2 cm margins to prevent recurrence, the only established treatment.
The patient has not yet undergone surgery and remains under regular follow-up. At the most recent evaluation, the lesions showed no significant changes.
COMMENTS
MPM is an uncommon presentation of PM, defined by the progressive appearance of new lesions over time.(5) The clinical course observed in this patient, characterized by the emergence of lesions in different anatomical regions over several years, supports this pattern and is consistent with previous descriptions of MPM. Recurrence of PM has been associated with incomplete excision.(8) However, the pattern observed in this patient cannot be fully explained by local recurrence, as new lesions appeared in different regions following complete excision of previous lesions. This finding suggests a multifocal process in addition to the possibility of local recurrence, rather than attributing all lesions to surgical failure, as described in recent literature.(6,8)
Although MPM is considered rare, representing a small proportion of cases,(4,5) the progressive development documented in this patient broadens the clinical spectrum in the pediatric population. MPM has been associated with underlying biological mechanisms or syndromes; however, in this case, no neurological or systemic findings were identified, supporting the existence of isolated MPM without associated comorbidities.(4,6)
The diagnosis of PM is predominantly clinical and supported by imaging studies, with ultrasound playing a key role in identifying calcified nodules.(7) In this patient, imaging findings were consistent with those described in the literature, and histopathological confirmation of excised lesions demonstrated basaloid cells, shadow (ghost) cells, and calcification, which remain the defining features of PM.(2,7) The combination of clinical signs, including a positive tent sign, imaging findings, and histology strengthens diagnostic certainty in MPM cases.
PM generally carries a benign prognosis;(9) however, in rare cases, a malignant variant—pilomatrix carcinoma—may develop.(10) To date, no cases of malignancy have been reported in MPM. These considerations highlight the importance of long-term follow-up to monitor for potential complications.
This case underscores the importance of recognizing multiple as a condition that may involve both recurrent lesions and multifocal disease processes. While recurrence is typically associated with incomplete excision, the development of lesions in anatomically distinct regions suggests an additional multifocal mechanism. Recognizing the coexistence of these processes is essential to avoid misinterpretation as surgical failure and to guide appropriate long-term surveillance strategies.
Ethics and Consent
Written informed consent was obtained from the patient’s legal guardian for the publication of this case and its associated images, in accordance with the principles of the Declaration of Helsinki.
BIBLIOGRAPHIC REFERENCES
1. Hu JL, Yoo H, Kwon ST, Kim S, Chung JH, Kim H, et al. Clinical analysis and review of literature on pilomatrixoma in pediatric patients [Internet]. Arch Craniofac Surg. 2020;21(5):288–93. DOI: 10.7181/acfs.2020.00528
2. Mohr C, Tschen J. Atypical pediatric presentation of pilomatricoma [Internet]. Cureus. 2023;15(6):e39909. DOI: 10.7759/cureus.39909
3. Lu C, Zhang R, Bi L, Luo T, Lai W, Fan W, Jing H. Clinical Features, Diagnostic Challenges, and Therapeutic Outcomes of 105 Pilomatricoma Cases [Internet]. Clin Cosmet Investig Dermatol. 2025;18:1801-1807. DOI: 10.2147/CCID.S518408
4. Chan JJ, Tey HL. Multiple pilomatricomas: case presentation and review of the literature [Internet]. Dermatol Online J. 2010;16(4):2. DOI: 10.5070/D31td0145c
5. Mesa-Álvarez L, Batalla A, Iglesias-Puzas Á, Álvarez C, Flórez Á. Multiple pilomatricomas: a retrospective study and literature review [Internet]. Am J Dermatopathol. 2019;41(4):293–5. DOI: 10.1097/DAD.0000000000001296
6. Chessa MA, Baracca MF, Rossi AN, Piraccini BM, De Pietro V, Picciola VM, et al. Pilomatricoma: Clinical, Dermoscopic Findings and Management in 55 Pediatric Patients and Concise Review of the Literature with Special Emphasis on Dermoscopy [Internet]. Dermatol Pract Concept. 2024;14(2):e2024140. DOI: 10.5826/dpc.1402a140
7. Bulman JC, Ulualp SO, Rajaram V, Koral K. Pilomatricoma of Childhood: A Common Pathologic Diagnosis Yet a Rare Radiologic One [Internet]. American Journal of Roentgenology. 2015;206(1):182–8. DOI:10.2214/AJR.15.14842
8. Saponaro G, De Paolis E, Todaro M, Azzuni F, Gasparini G, Bosso A, et al. Pilomatricoma in Syndromic Contexts: A Literature Review and a Report of a Case in Apert Syndrome [Internet]. Dermatopathology. 2025;12(3):24. DOI: 10.3390/dermatopathology12030024
9. Cornejo KM, Deng A. Pilomatrix carcinoma: a case report and review of the literature [Internet]. Am J Dermatopathol. 2013;35(3):389–94. DOI: 10.1097/DAD.0b013e318274b7da
10. Dang J, Sun J, Wang W, Zhang Y. Pilomatricoma in the right parotid region: A case report and review of the literature [Internet]. Asian J Surg. 2023;46(6):2393-2394. DOI: 10.1016/j.asjsur.2022.12.029
Conflicts of Interest
The authors have no conflicts of interest to declare.
Financial Information
Not applied.
Data Availability
The data used for this case report correspond to the Hospital Nacional San José de Chincha, Ica – Perú.